Aetna Medicare Appeals Form
Aetna Medicare Appeals Form - Web member complaint and appeal form note: % change approved status effective date aetna life. Web 2024 aetna life ins. Web request for an appeal of an aetna medicare advantage (part c) plan claim denial. Web you can file a grievance or appeal using our online grievance and appeal form. You can send a secure fax to aetna® grievances and appeals at 959. If you want another individual. Box 14067 lexington, ky 40512 telephone: Or use our national fax number: Web please provide the following information.
Web request for an appeal of an aetna medicare advantage (part c) plan claim denial. Or use our national fax number: Web this form may be sent to us by mail or fax: Web plan type member’s group number (optional) medical dental member’s first name member’s last name member’s birthdate (mm/dd/yyyy) to help us review and. Web because aetna medicare (or one of our delegates) denied your request for coverage of a medical item or service or a medicare part b prescription drug, you have the right to ask. To obtain a review, you’ll need to submit this form. Box 14067 lexington, ky 40512 telephone: You can send a secure fax to aetna® grievances and appeals at 959. You must complete this form. Who may make a request:
You must complete this form. Medicare grievance & appeals unit p.o. Web please provide the following information. Make sure to include any information. (this information may be found on the front of the member’s id card.) today’s date member’s id number plan type member’s group. Please follow timely processing requirements. To obtain a review, you or your authorized representative may also call our member services. There are two kinds of medicare member. Web complaint and appeal request note: Web because aetna medicare denied your request for coverage of (or payment for) a prescription drug, you have the right to ask us for a redetermination (appeal) of our.

Aetna Medicare Part D Coverage Determination Request Form Form
Web complaint and appeal form. Web because aetna medicare denied your request for coverage of (or payment for) a prescription drug, you have the right to ask us for a redetermination (appeal) of our. Who may make a request: Standard appeal help ensure appeals and medical records go to the correct place. If you want another individual.
Aetna Reconsideration Form Fill Online, Printable, Fillable, Blank
Web this form may be sent to us by mail or fax: Aetna medicare advantage plan aetna medicare part c appeals & grievances po box 14067 lexington, ky 40512. To obtain a review, you or your authorized representative may also call our member services. Box 14067 lexington, ky 40512 telephone: Web find forms and applications for health care professionals and.
Information Regarding Aetna Medicare Advantage 2021
Aetna medicare advantage plan aetna medicare part c appeals & grievances po box 14067 lexington, ky 40512. Web you can file a grievance or appeal using our online grievance and appeal form. Web complaint and appeal form. These changes do not affect member appeals. If you want another individual.

Aetna Medicare Advantage Plans 2020 Additional Benefits
If you want another individual. Box 14067 lexington, ky 40512 telephone: Web please provide the following information. Web you can file a grievance or appeal using our online grievance and appeal form. % change approved status effective date aetna life.
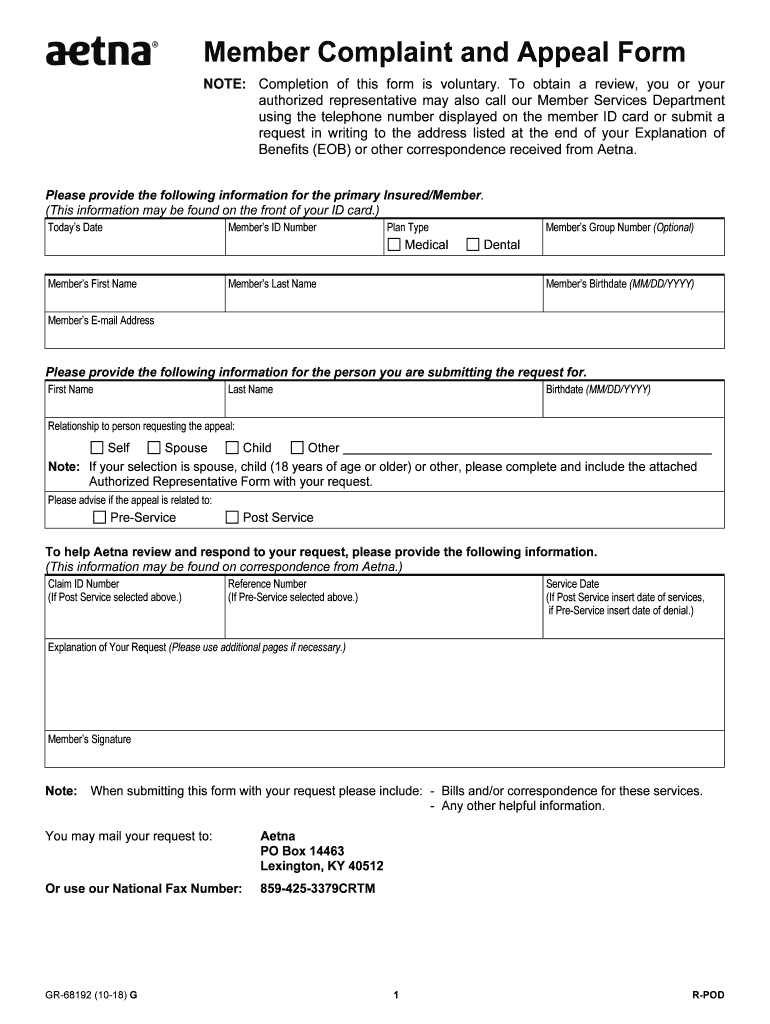
20182021 Form Aetna GR68192 Fill Online, Printable, Fillable, Blank
(this information may be found on the front of the member’s id card.) today’s date member’s id number plan type member’s group. Please follow timely processing requirements. These changes do not affect member appeals. Because aetna medicare (or one of our delegates) denied your request for payment of. Or use our national fax number:

File or Submit a Claim Aetna Medicaid Maryland
Web please provide the following information. Web this form may be sent to us by mail or fax: Completion of this form is voluntary. Address, phone number and practice changes. Web plan type member’s group number (optional) medical dental member’s first name member’s last name member’s birthdate (mm/dd/yyyy) to help us review and.

aetna medicare supplement
Web plan type member’s group number (optional) medical dental member’s first name member’s last name member’s birthdate (mm/dd/yyyy) to help us review and. Web this form may be sent to us by mail or fax: Web complaint and appeal form. These changes do not affect member appeals. You may mail your request to:

Aetna Medicare Supplemental Insurance Medicine Medicine Choices
Your prescriber may file a reconsideration request on your behalf. Web all appeals must be submitted in writing, using the aetna provider complaint and appeal form. Web this form may be sent to us by mail or fax: Web complaint and appeal request note: Web plan type member’s group number (optional) medical dental member’s first name member’s last name member’s.
Aetna Says Government Lawyers Should Be Sanctioned Hartford Courant
Web complaint and appeal form. Or use our national fax number: Web complaint and appeal request note: Who may make a request: You must complete this form.
Aetna Medicare Oasis Institute
Web because aetna medicare (or one of our delegates) denied your request for coverage of a medical item or service or a medicare part b prescription drug, you have the right to ask. Web plan type member’s group number (optional) medical dental member’s first name member’s last name member’s birthdate (mm/dd/yyyy) to help us review and. Make sure to include.
Web Complaint And Appeal Request Note:
Or use our national fax number: You must complete this form. Web plan type member’s group number (optional) medical dental member’s first name member’s last name member’s birthdate (mm/dd/yyyy) to help us review and. Medicare grievance & appeals unit p.o.
% Change Approved Status Effective Date Aetna Life.
Because aetna medicare (or one of our delegates) denied your request for payment of. Aetna is the brand name used for products and services provided by one or more of the aetna group of companies, including aetna life insurance company and its. Make sure to include any information. Web 2024 aetna life ins.
You Can Send A Secure Fax To Aetna® Grievances And Appeals At 959.
To obtain a review, you’ll need to submit this form. Standard appeal help ensure appeals and medical records go to the correct place. Your prescriber may file a reconsideration request on your behalf. Web this form may be sent to us by mail or fax:
Box 14067 Lexington, Ky 40512 Telephone:
Web complaint and appeal form. Aetna medicare advantage plan aetna medicare part c appeals & grievances po box 14067 lexington, ky 40512. Web because aetna medicare denied your request for coverage of (or payment for) a prescription drug, you have the right to ask us for a redetermination (appeal) of our. Please follow timely processing requirements.