Bcbs Name Change Form
Bcbs Name Change Form - Web in section 4, please include enrollee’s or dependent’s name, social security number, date of birth, and name and number of the new pcp. Web the following changes can be submitted: Social security number (if no ss#, write n/a) gender q male date of birth (month/day/year) Web use this form for owners to attest for eligibility. Web enrollment and change form. Web change of status form for group plans. Web register now, or download the sydney health app to access your benefits, id card, pharmacy info, and more. If your wife signs up for her plan directly through us she can contact us by. 22nd street, lombard, illinois 60148. Web changes you can make using the demographic change form include:
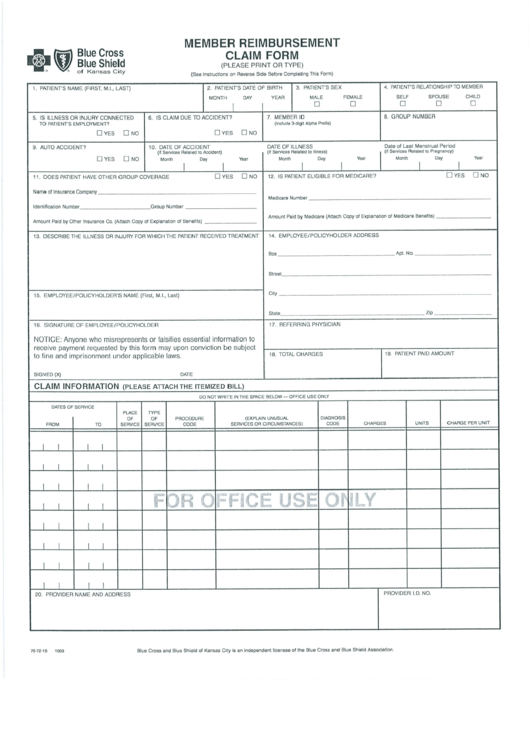
Web enrollee’s or dependent’s name, social security number, date of birth, name and number of the new pcp and the name and number of the new ipa. Web change of status form. Download (fillable pdf) group change request. Web register now, or download the sydney health app to access your benefits, id card, pharmacy info, and more. All required documentation is attached. Blue cross and blue shield global core international claims. Web change of status form for group plans. Web if you purchase insurance individually (not through an employer) and need to make a change, please call us at 800‑280‑2583. If you get your insurance through work, please. Products issued by dearborn life insurance company, 701 e.
Prefer to submit your health insurance claim by. Web the following forms can be found inside your mybluekc portal: Web change forms if you are already enrolled but need to change things such as provider name, contact information, office hours, panel status, or hospital affiliations, please fill. 22nd street, lombard, illinois 60148. If your wife signs up for her plan directly through us she can contact us by. Web use this form for owners to attest for eligibility. Products issued by dearborn life insurance company, 701 e. Blue cross and blue shield global core international claims. For blue cross blue shield of michigan mail: Web include enrollee’s or dependent’s name, social security number, date of birth, and name and number of the new pcp.
Fillable Bcbsaz Corrected Claim Form printable pdf download
Web the following changes can be submitted: Electronic data interchange (edi) quality of care incident form. Web change forms if you are already enrolled but need to change things such as provider name, contact information, office hours, panel status, or hospital affiliations, please fill. If you get your insurance through work, please. If your wife signs up for her plan.
Bcbs Enrollment Change Request Form
Blue cross and blue shield global core international claims. Web if you purchase insurance individually (not through an employer) and need to make a change, please call us at 800‑280‑2583. Web include enrollee’s or dependent’s name, social security number, date of birth, and name and number of the new pcp. If you get your health plan through your employer, you.
Bcbs Of Alabama Prior Authorization Fill Out and Sign Printable PDF
Electronic data interchange (edi) quality of care incident form. Web provider manual and guides. Web changes you can make using the demographic change form include: Download (fillable pdf) group change request. Complete section 1 and check the.
Bcbs Alabama Prior Authorization Form Fill Out and Sign Printable PDF
Web if you purchase insurance individually (not through an employer) and need to make a change, please call us at 800‑280‑2583. Prefer to submit your health insurance claim by. Web enrollment and change form. Web provider manual and guides. Web use this form for owners to attest for eligibility.

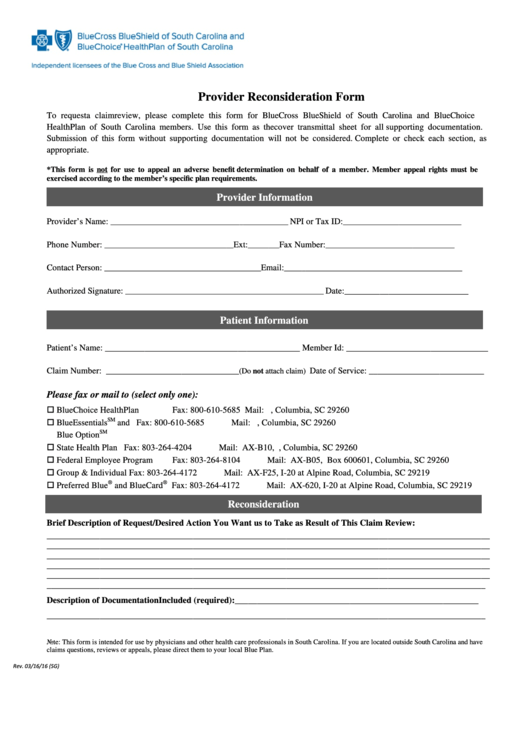
Bcbs Claim Review Form mekabdesigns
Download (fillable pdf) group change request. If you get your insurance through work, please. Web first name mi last name relationship to you? Web the following changes can be submitted: Web provider manual and guides.

Bcbs Name Change Form
Understand your care options ahead of time so you can save. Social security number (if no ss#, write n/a) gender q male date of birth (month/day/year) Web include enrollee’s or dependent’s name, social security number, date of birth, and name and number of the new pcp. Blue cross and blue shield global core international claims. Web the following changes can.
270 Bcbs Forms And Templates free to download in PDF
Web register now, or download the sydney health app to access your benefits, id card, pharmacy info, and more. This form replaces the “request for contract change”, the “group. For blue cross blue shield of michigan mail: Web in section 4, please include enrollee’s or dependent’s name, social security number, date of birth, and name and number of the new.

Bcbs Federal Provider Appeal form Best Of File Plaint Blue Shield
Web the following changes can be submitted: Download (fillable pdf) group change request. Social security number (if no ss#, write n/a) gender q male date of birth (month/day/year) 22nd street, lombard, illinois 60148. Web enrollee’s or dependent’s name, social security number, date of birth, name and number of the new pcp and the name and number of the new ipa.
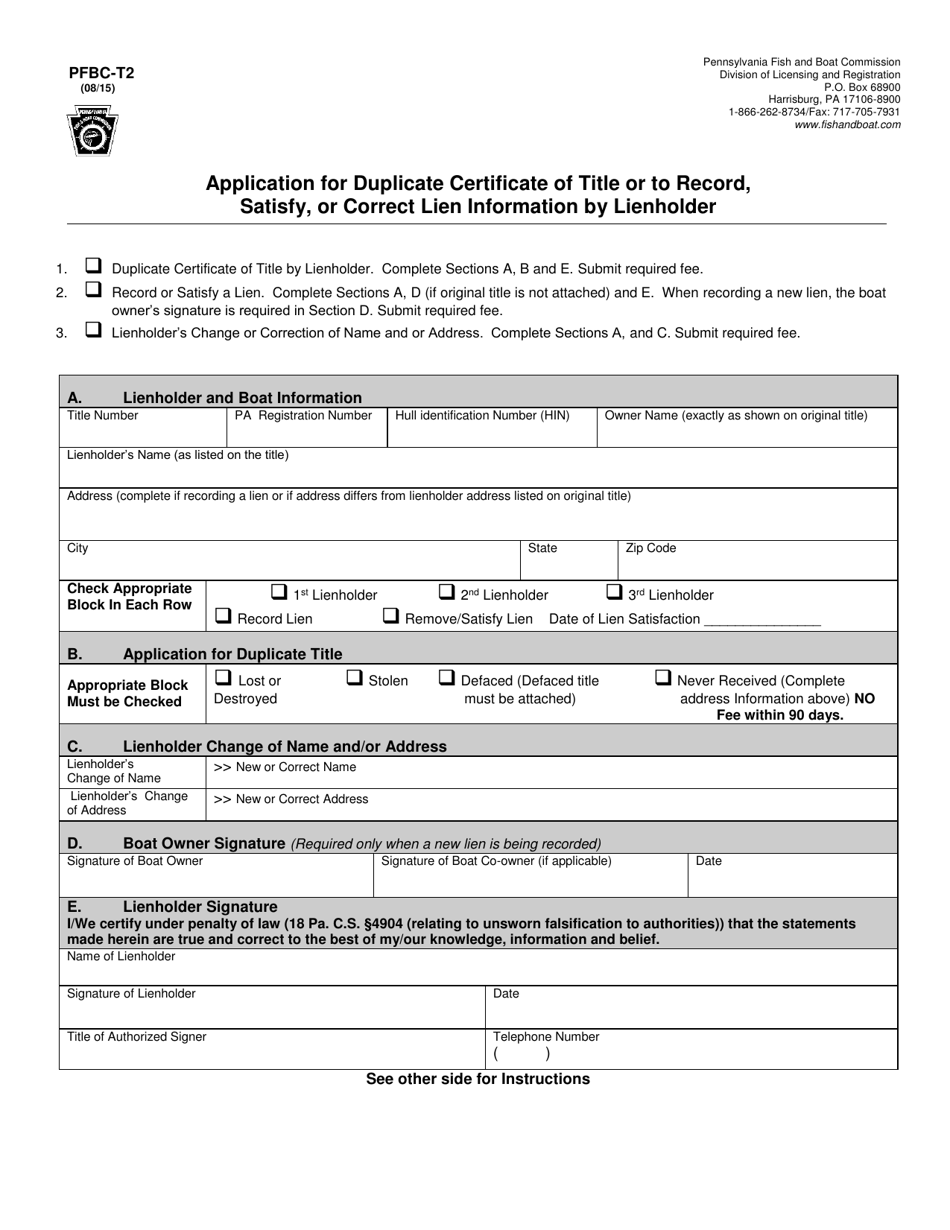
Application For Tax Clearance Certificate Pa Instructions How To Get
Social security number (if no ss#, write n/a) gender q male date of birth (month/day/year) Web change of status form. Blue cross and blue shield global core international claims. Complete section 1 and check the. For blue cross blue shield of michigan mail:
Bcbs Claim Review Form mekabdesigns
Web use this form for owners to attest for eligibility. Products issued by dearborn life insurance company, 701 e. Web provider manual and guides. If you get your insurance through work, please. All required documentation is attached.
If You Get Your Health Plan Through Your Employer, You Can Use This Form To Update Us When You Have Any Changes To Your Status.
Web hello, yes, we can change a member's name and issue new id cards if there is a name change. Web provider manual and guides. If you get your insurance through work, please. Web change forms if you are already enrolled but need to change things such as provider name, contact information, office hours, panel status, or hospital affiliations, please fill.
Download (Fillable Pdf) Group Change Request.
Web enrollee’s or dependent’s name, social security number, date of birth, name and number of the new pcp and the name and number of the new ipa. Web in section 4, please include enrollee’s or dependent’s name, social security number, date of birth, and name and number of the new pcp. Web the following forms can be found inside your mybluekc portal: All required documentation is attached.
Web Changes You Can Make Using The Demographic Change Form Include:
Web if you purchase insurance individually (not through an employer) and need to make a change, please call us at 800‑280‑2583. Electronic data interchange (edi) quality of care incident form. Products issued by dearborn life insurance company, 701 e. Web include enrollee’s or dependent’s name, social security number, date of birth, and name and number of the new pcp.
Blue Cross And Blue Shield Global Core International Claims.
Web use this form for owners to attest for eligibility. This form replaces the “request for contract change”, the “group. Prefer to submit your health insurance claim by. 22nd street, lombard, illinois 60148.