Carefirst Termination Form
Carefirst Termination Form - Medical, dental, vision coverage if you enrolled directly through carefirst. Web reinstatement request form and make payment of all past and currently due premiums. Payment of all amounts due is required. Box 14651, lexington, ky 40512fax: Minor vaccination consent notification form. Days from the date of your termination letter. Do it online, fast & easy. Ad need to terminate your carefirst contract? Web plan termination view form (applies to all plans) proof of coverage social security number submission form Medical, dental coverage if you enrolled via the maryland or dc health exchanges.
Web plan termination view form (applies to all plans) proof of coverage social security number submission form Web request for continuity of care for new members (pdf) medplus household discount request form. You must submit a payment of all past and currently due premiums in full. For residents of maryland who purchased a medplus medigap plan with an effective date of august 1, 2016 or later. Web reinstatement request form and make payment of all past and currently due premiums. View form (applies to all plans) plan termination. This form and your payment must. Inmediate delivery of your cancellation letter with proof of mailing. Payment of all amounts due is required. Days from the date of your termination letter.
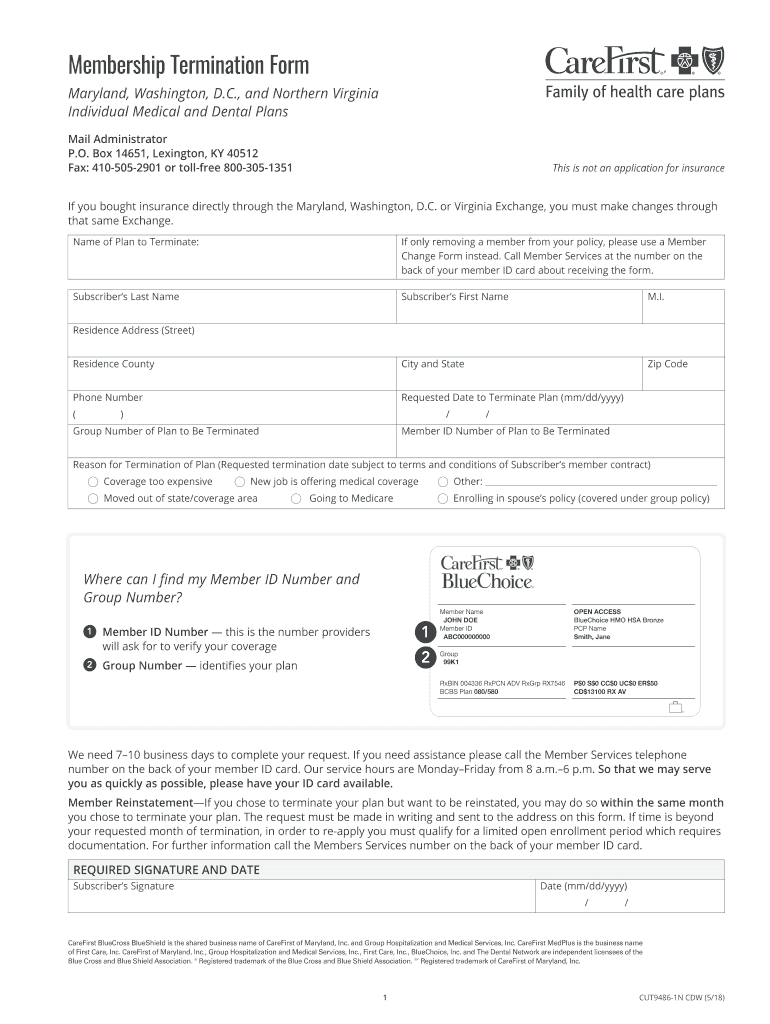
This form and your payment must. View form (applies to all plans) plan termination. Web membership termination form maryland, district of columbia and northern virginia individual plans mailroom administrator p.o. Web request for continuity of care for new members (pdf) medplus household discount request form. Payment of all amounts due is required. For residents of maryland who purchased a medplus medigap plan with an effective date of august 1, 2016 or later. Box 14651, lexington, ky 40512fax: This form cannot be used to cancel the following health insurance coverage: Minor vaccination consent notification form. View form (applies to all plans) disability certification.
Carefirst Termination Form Fill Out and Sign Printable PDF Template
View form (applies to all plans) plan termination. View form (applies to all plans) disability certification. Web membership termination form maryland, district of columbia and northern virginia individual plans mailroom administrator p.o. Payment of all amounts due is required. Do it online, fast & easy.
Carefirst Medical Claim Form Fill Out and Sign Printable PDF Template
View form (applies to all plans) plan termination. Web membership termination form maryland, district of columbia and northern virginia individual plans mailroom administrator p.o. Medical, dental, vision coverage if you enrolled directly through carefirst. Inmediate delivery of your cancellation letter with proof of mailing. Web use this form to cancel the following health insurance coverage:
Carefirst Eft Enrollment Fill Out and Sign Printable PDF Template
Web plan termination view form (applies to all plans) proof of coverage social security number submission form This form and your payment must. View form (applies to all plans) plan termination. Days from the date of your termination letter. Web request for continuity of care for new members (pdf) medplus household discount request form.
Carefirst Referral Form Fill Out and Sign Printable PDF Template
Payment of all amounts due is required. Ad need to terminate your carefirst contract? View form (applies to all plans) proof of coverage. Do it online, fast & easy. This form and your payment must.
Termination form Template Free Of Termination Notice to Employee format
Web use this form to cancel the following health insurance coverage: Web this form is used to request that your insurer terminate the restriction on your protected health information (phi). Web for questions concerning your membership and benefits, or to obtain other fep forms, contact member services at the telephone number on your id card or visit www.fepblue.org. Days from.
Carefirst Vision Claim Form Fill Out and Sign Printable PDF Template
Web plan termination view form (applies to all plans) proof of coverage social security number submission form Medical, dental coverage if you enrolled via the maryland or dc health exchanges. Ad need to terminate your carefirst contract? Web for questions concerning your membership and benefits, or to obtain other fep forms, contact member services at the telephone number on your.
Maryland Uniform Referral Form Fill Out and Sign Printable PDF
This form cannot be used to cancel the following health insurance coverage: Inmediate delivery of your cancellation letter with proof of mailing. View form (applies to all plans) proof of coverage. Payment of all amounts due is required. Be received by carefirst no later than.
Carefirst Termination Form Fill Out and Sign Printable PDF Template
View form (applies to all plans) disability certification. Web request for continuity of care for new members (pdf) medplus household discount request form. Medical, dental coverage if you enrolled via the maryland or dc health exchanges. Web this form is used to request that your insurer terminate the restriction on your protected health information (phi). You must submit a payment.

AZ Care1st Health Plan Treatment Authorization Request 2012 Fill and
Web plan termination view form (applies to all plans) proof of coverage social security number submission form You must submit a payment of all past and currently due premiums in full. Inmediate delivery of your cancellation letter with proof of mailing. Web reinstatement request form and make payment of all past and currently due premiums. View form (applies to all.
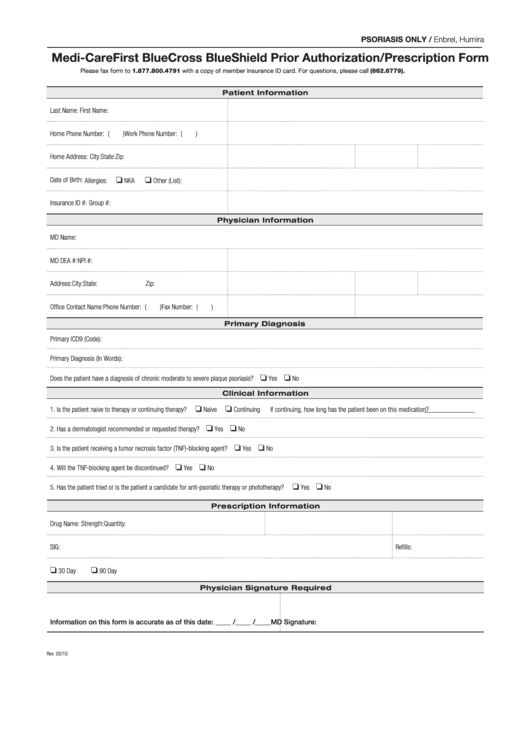
Fillable MediCarefirst Bluecross Blueshield Prior Authorization
Do it online, fast & easy. Ad need to terminate your carefirst contract? View form (applies to all plans) disability certification. Web membership termination form maryland, district of columbia and northern virginia individual plans mailroom administrator p.o. Box 14651, lexington, ky 40512fax:
Web This Form Is Used To Request That Your Insurer Terminate The Restriction On Your Protected Health Information (Phi).
Medical, dental coverage if you enrolled via the maryland or dc health exchanges. Web membership termination form maryland, district of columbia and northern virginia individual plans mailroom administrator p.o. Do it online, fast & easy. For residents of maryland who purchased a medplus medigap plan with an effective date of august 1, 2016 or later.
Web Use This Form To Cancel The Following Health Insurance Coverage:
Protected health information (phi) authorization form for information release. Web for questions concerning your membership and benefits, or to obtain other fep forms, contact member services at the telephone number on your id card or visit www.fepblue.org. View form (applies to all plans) disability certification. View form (applies to all plans) plan termination.
View Form (Applies To All Plans) Proof Of Coverage.
Web plan termination view form (applies to all plans) proof of coverage social security number submission form Minor vaccination consent notification form. Medical, dental, vision coverage if you enrolled directly through carefirst. Be received by carefirst no later than.
This Form Cannot Be Used To Cancel The Following Health Insurance Coverage:
Ad need to terminate your carefirst contract? Inmediate delivery of your cancellation letter with proof of mailing. Days from the date of your termination letter. Payment of all amounts due is required.