Dental Patient Registration Form Pdf
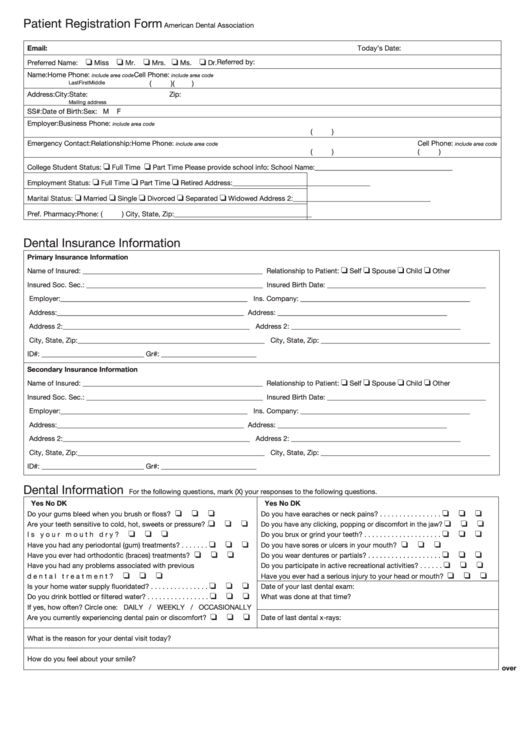
Dental Patient Registration Form Pdf - Date relationship to patient 1 patient information 2 dental insurance. Web patient registration form american dental association www.ada.org dental insurance information dental information for the following questions, mark (x) your responses to the following questions. Secure, online patient registration for your website. D.o.b social security # street address: Web family physicians of kansas patient registration form we are required to capture demographic data including your preferred language, race and ethnicity. On your patient registration form? Web dental registration and history. Web a dental patient information form is used by dental practices for collecting information about patients before the appointment. Web patient registration form sf820 clinicas del camino real, inc. This is an important part of your medical history and will assist us during our clinical quality improvement process.
Dental appointment policy in an effort to ensure access for all our dental patients. Sign online button or tick the preview image of. Dental insurance rarely covers all fees; Please complete the information below. Web dental registration form ‐ adult updated 2/2018 disclosure of protected health information this form is to protect your consent to use or disclose your protectd health information 1. D.o.b social security # street address: I, the undersigned, certify that i (or my dependent) have insurance coverage and assign all insurance benefits directly to prohealth dental that are otherwise payable to me for services rendered. Appointment information yes ____ no ____ Tips on how to complete the patient registration form.pdf on the web: What you prefer to be called:
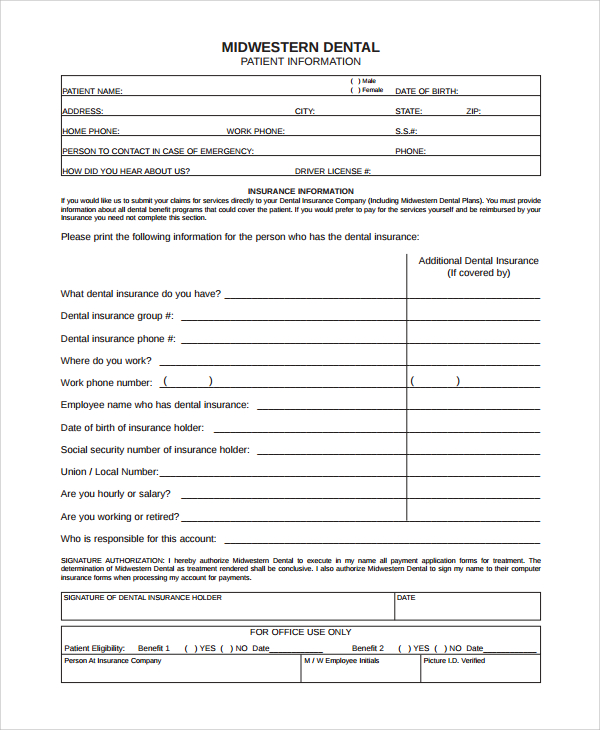
Or do not take because of errors or omissions that i may have made in the completion of this form. Dental appointment policy in an effort to ensure access for all our dental patients. Web patient registration form 1120 e. This dental patient information form allows new patients to enroll your database by providing their personal and contact information, dental insurance details, health information with further details. This is an important part of your medical history and will assist us during our clinical quality improvement process. I acknowledge that my questions have been answered to my satisfaction. Web dental registration form ‐ adult updated 2/2018 disclosure of protected health information this form is to protect your consent to use or disclose your protectd health information 1. Web the dental group submits insurance claims solely to primary dental insurance for patients’ convenience and does not assume responsibility for the processing of such insurance or failure of insurance to pay for any reason. For examples, refer to our sample medical consent forms. Web complete your patient forms in advance of your appointment.

Dental Patient Registration form Template Lovely 27 Of Dental New
Save time and resources by completing the registration process of your patients with this online form. Web patient registration form 1120 e. Twenty four (24) to forty eight (48. I acknowledge that my questions have been answered to my satisfaction. Physician’s name_____ date of last visit _____ have you ever used a bisphosphonate medication?

Dental Patient Registration form Template Best Of Medical History form
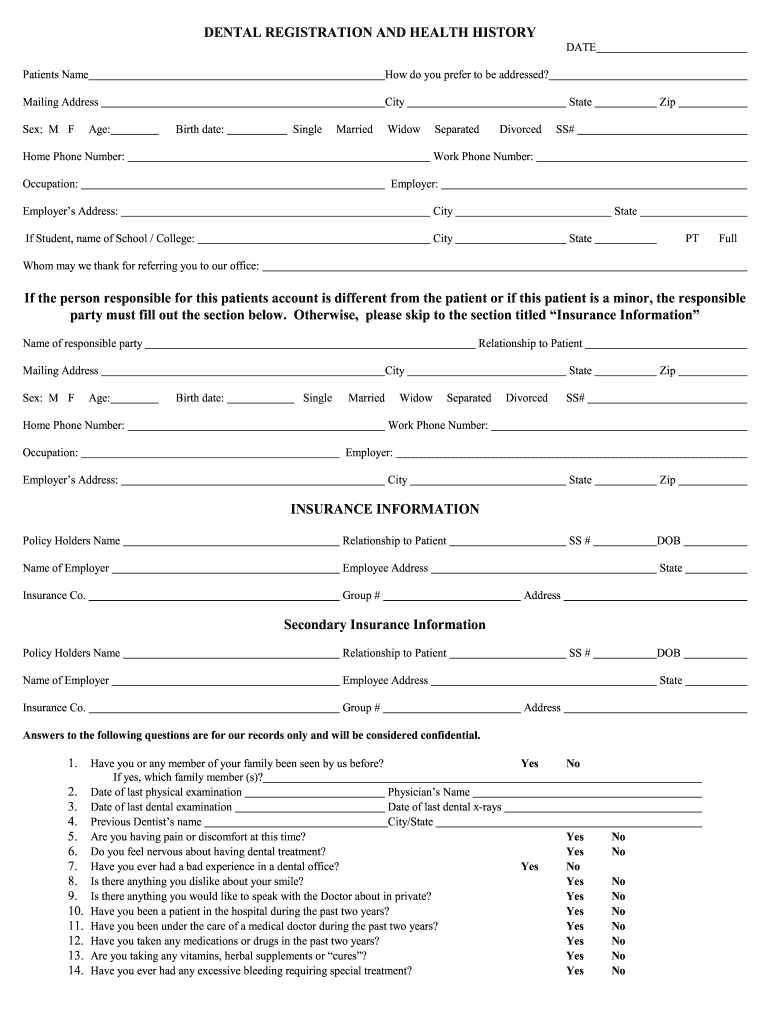
Web patient registration form (formulario de registro del paciente) patient information (información del paciente): Download free version (pdf format) download editable version for $3.99 (word format) download the entire collection for only $99 what's the difference? Web dental registration and history. Sale of dental practice form download pdf. Web dental registration form ‐ adult updated 2/2018 disclosure of protected health.
Patient Registration Form American Dental Association printable pdf
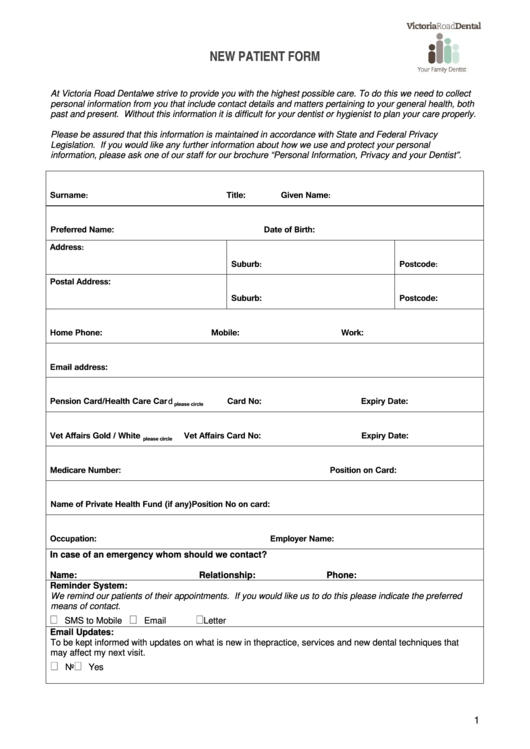
Web a dental patient information form is used by dental practices for collecting information about patients before the appointment. Direct deposit enrollment form download pdf. Dental insurance rarely covers all fees; This dental patient information form allows new patients to enroll your database by providing their personal and contact information, dental insurance details, health information with further details. This is.

New Patient Forms Steeplechase Dental
This is an important part of your medical history and will assist us during our clinical quality improvement process. Save time and resources by completing the registration process of your patients with this online form. The form is available in a digital, downloadable version or in print. I understand that i am financially responsible for all Direct deposit enrollment form.
Dental Patient Form printable pdf download
Web landon state office building. Individual patient (or personal representative) confirming the consent Web the dental group submits insurance claims solely to primary dental insurance for patients’ convenience and does not assume responsibility for the processing of such insurance or failure of insurance to pay for any reason. I understand that i am financially responsible for all Appointment information yes.
Dental Registration And History Form 20202021 Fill and Sign
Save time and resources by completing the registration process of your patients with this online form. Web employer account registration form download pdf. Web patient registration form today’s date: On your patient registration form? I understand that i am financially responsible for all
FREE 8+ Sample Patient Registration Forms in PDF MS Word
Email address (dirección de correo electrónico): Patient registration form american dental association www.ada.org dental insurance information dental information for the following questions, mark (x) your responses to the following questions. Web a dental patient information form is used by dental practices for collecting information about patients before the appointment. Single married divorced child other first name: Dental appointment policy in.

Dental Patient Registration form Template Luxury Best S Of Printable
Tips on how to complete the patient registration form.pdf on the web: Date relationship to patient 1 patient information 2 dental insurance. Web the american dental association (ada) offers a comprehensive health history form, for adults or children in both english and spanish, that covers both medical and dental issues. Web patient registration form today’s date: I will not hold.

printable dental patient registration form template sample in 2021
The form is available in a digital, downloadable version or in print. Web patient registration form today’s date: Web patient registration form sf820 clinicas del camino real, inc. Web patient registration form 1120 e. Web the dental group submits insurance claims solely to primary dental insurance for patients’ convenience and does not assume responsibility for the processing of such insurance.
FREE 9+ Patient Registration Form Samples in PDF Excel MS Word
Web landon state office building. Web patient’s relationship to subscriber: Dental appointment policy in an effort to ensure access for all our dental patients. Or do not take because of errors or omissions that i may have made in the completion of this form. Web the american dental association (ada) offers a comprehensive health history form, for adults or children.
Secure, Online Patient Registration For Your Website.
To begin the document, use the fill camp; Web patient’s relationship to subscriber: Web a dental patient information form is used by dental practices for collecting information about patients before the appointment. What you prefer to be called:
D.o.b Social Security # Street Address:
I, the undersigned, certify that i (or my dependent) have insurance coverage and assign all insurance benefits directly to prohealth dental that are otherwise payable to me for services rendered. This is an important part of your medical history and will assist us during our clinical quality improvement process. Web dental registration and history. Email address (dirección de correo electrónico):
Web Patient Registration Form (Formulario De Registro Del Paciente) Patient Information (Información Del Paciente):
Sign online button or tick the preview image of. Appointment information yes ____ no ____ Web new patient registration form patient personal information title last, first address nickname city, state, zip email health care guardian name health care guardian phone # birth date marital status home # cell # emergency contact student school name referral type age sex work # drive lic emergency phone # ssn Tips on how to complete the patient registration form.pdf on the web:
Individual Patient (Or Personal Representative) Confirming The Consent
Single married divorced child other first name: (06/2020) page 1 patient information last name: I acknowledge that my questions have been answered to my satisfaction. I understand that i am financially responsible for all