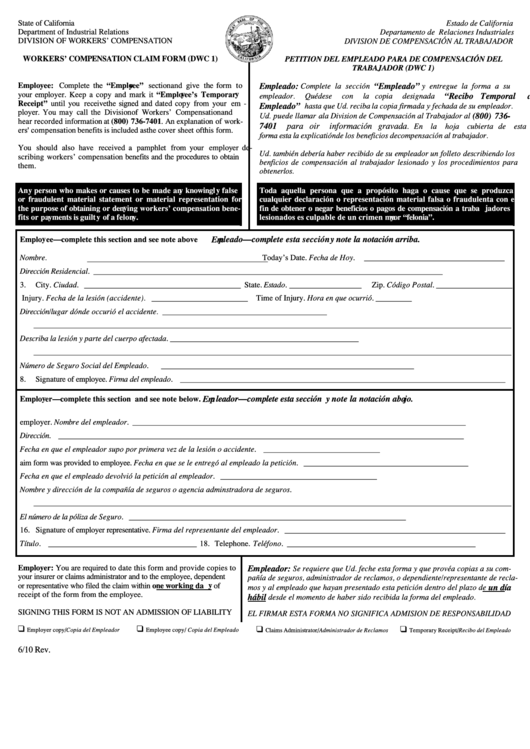
Dwc-1 Form
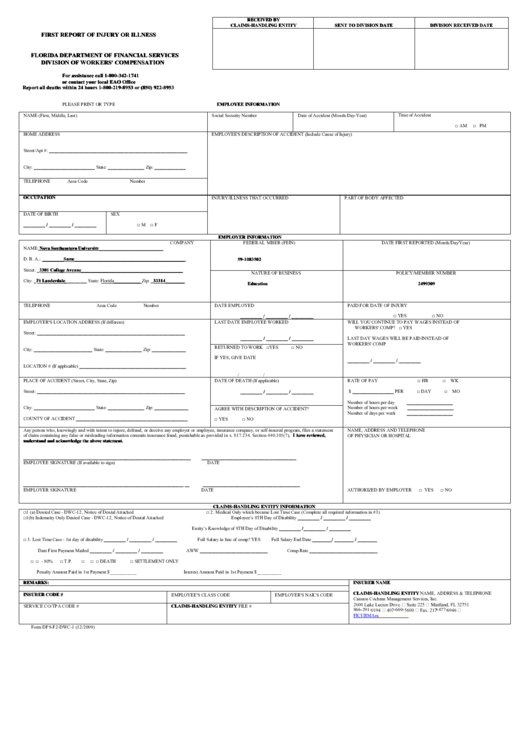
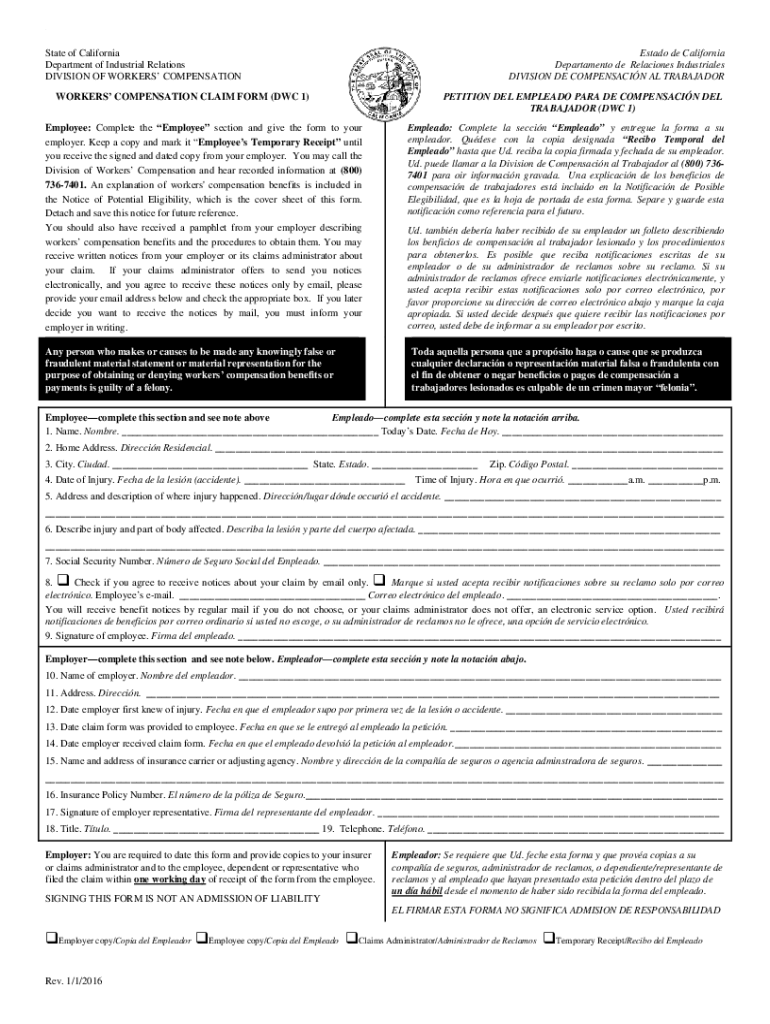
Dwc-1 Form - Bona fide offer of employment letter (sample, english) doc. Number workers' compensation claim form. You should read all of the information. The social security number will be used as a unique identifier in division of workers' compensation database systems for individuals who have claimed benefits under Claims and return to work. Use the attached form to file a workers’ compensation claim with your employer. The collection of the social security number on this form is. You should read all of the information below. Web the employer's first report of injury or illnessprovides information on the claimant, employer, insurance carrier and medical practitioner necessary to begin the claims process. Details of the claimant's employment and circumstances surrounding the injury or illness are also requested.
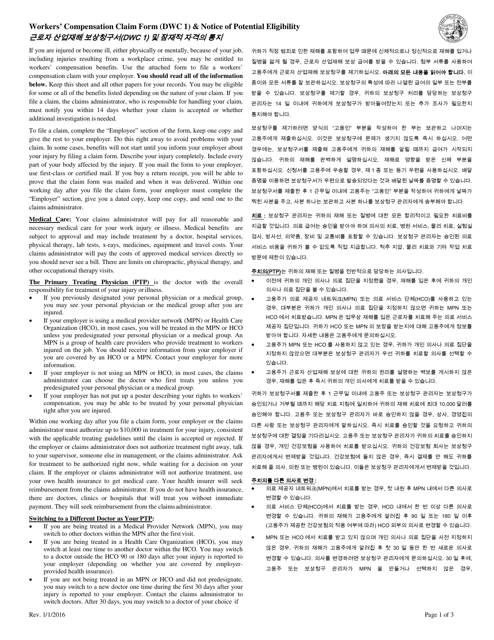
Employer's report of occupational injury or illness: If you are injured or become ill, either physically or mentally, because of your job, including injuries resulting from a workplace crime, you may be entitled to workers’ compensation benefits. Bona fide offer of employment letter (sample, english) doc. Claims and return to work. The social security number will be used as a unique identifier in division of workers' compensation database systems for individuals who have claimed benefits under Uninsured employer name (please leave blank spaces between numbers, names or words) employer street address/po box (please leave blank spaces between numbers, names or words) Details of the claimant's employment and circumstances surrounding the injury or illness are also requested. You may be eligible for some or all of the benefits listed depending on the nature of your claim. The collection of the social security number on this form is. However, the following items may require more attention:
Web find common forms used during the claims process and throughout your policy period. If you are injured or become ill, either physically or mentally, because of your job, including injuries resulting from a workplace crime, you may be entitled to workers’ compensation benefits. Web the employer's first report of injury or illnessprovides information on the claimant, employer, insurance carrier and medical practitioner necessary to begin the claims process. Claims and return to work. Number workers' compensation claim form. You may be eligible for some or all of the benefits listed depending on the nature of your claim. Web request an employee's claim for workers' compensation benefits form from your supervisor (it's also known as a dwc 1 form). Use the attached form to file a workers’ compensation claim with your employer. You should read all of the information. Use the attached form to file a workers’ compensation claim with your employer.
CA DWC Form 9783.1 2007 Fill and Sign Printable Template Online US
This information is no longer required. The collection of the social security number on this form is. 1/1/2016 page 1 of 3. You should read all of the information. Keep this sheet and all other papers for your records.

DWC 1 Form In the heights, Lift and carry, Compensation claim
However, the following items may require more attention: Employer's report of occupational injury or illness: Web find common forms used during the claims process and throughout your policy period. Your employer must give or mail you a claim form within one working day after learning about your injury or illness. Web the employer's first report of injury or illnessprovides information.
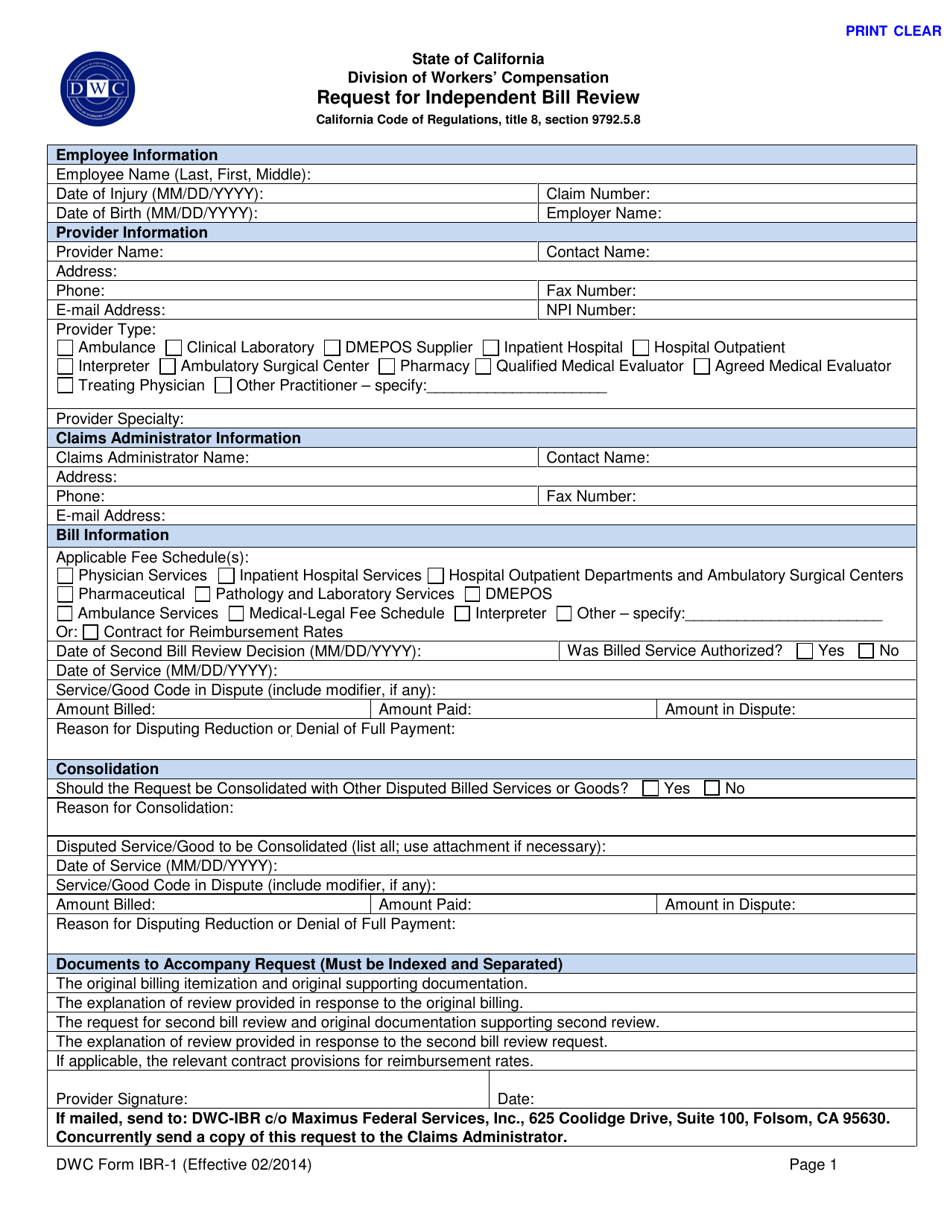
DWC Form IBR1 Download Fillable PDF or Fill Online Request for
You should read all of the information below. Web the employer's first report of injury or illnessprovides information on the claimant, employer, insurance carrier and medical practitioner necessary to begin the claims process. Claims and return to work. Web request an employee's claim for workers' compensation benefits form from your supervisor (it's also known as a dwc 1 form). Use.
Form Dwc 1 Workers' Compensation Claim Form printable pdf download
Use the attached form to file a workers’ compensation claim with your employer. If no home phone, please give a phone number where the employee can be reached. You may be eligible for some or all of the benefits listed depending on the nature of your claim. Employer's report of occupational injury or illness: The collection of the social security.
Fillable Form DfsF2Dwc1 First Report Of Injury Or Illness Template
Keep this sheet and all other papers for your records. You should read all of the information below. Use the attached form to file a workers’ compensation claim with your employer. Details of the claimant's employment and circumstances surrounding the injury or illness are also requested. Use the attached form to file a workers’ compensation claim with your employer.
Form DWC1 Fill Out, Sign Online and Download Printable PDF
Uninsured employer name (please leave blank spaces between numbers, names or words) employer street address/po box (please leave blank spaces between numbers, names or words) Web request an employee's claim for workers' compensation benefits form from your supervisor (it's also known as a dwc 1 form). Employer's report of occupational injury or illness: Keep this sheet and all other papers.
20162021 Form CA DIR DWC 1 Fill Online, Printable, Fillable, Blank
Specifically authorized by section 440.185(2), florida statutes. Bona fide offer of employment letter (sample, english) doc. This information is no longer required. However, the following items may require more attention: Keep this sheet and all other papers for your records.
Dwc 1 Claim Form mekabdesigns
Web the employer's first report of injury or illnessprovides information on the claimant, employer, insurance carrier and medical practitioner necessary to begin the claims process. If no home phone, please give a phone number where the employee can be reached. This information is no longer required. Web find common forms used during the claims process and throughout your policy period..
Dwc 25 Form Fill Out and Sign Printable PDF Template signNow
Web find common forms used during the claims process and throughout your policy period. Web the employer's first report of injury or illnessprovides information on the claimant, employer, insurance carrier and medical practitioner necessary to begin the claims process. You should read all of the information. You may be eligible for some or all of the benefits listed depending on.
DWC/WCAB Form 1A Download Fillable PDF or Fill Online Application for
This information is no longer required. Use the attached form to file a workers’ compensation claim with your employer. Specifically authorized by section 440.185(2), florida statutes. You should read all of the information. If no home phone, please give a phone number where the employee can be reached.
Web The Employer's First Report Of Injury Or Illnessprovides Information On The Claimant, Employer, Insurance Carrier And Medical Practitioner Necessary To Begin The Claims Process.
Web find common forms used during the claims process and throughout your policy period. Number workers' compensation claim form. Your employer must give or mail you a claim form within one working day after learning about your injury or illness. Claims and return to work.
Specifically Authorized By Section 440.185(2), Florida Statutes.
Use the attached form to file a workers’ compensation claim with your employer. Uninsured employer name (please leave blank spaces between numbers, names or words) employer street address/po box (please leave blank spaces between numbers, names or words) This information is no longer required. Use the attached form to file a workers’ compensation claim with your employer.
1/1/2016 Page 1 Of 3.
Bona fide offer of employment letter (sample, english) doc. You may be eligible for some or all of the benefits listed depending on the nature of your claim. You should read all of the information below. If no home phone, please give a phone number where the employee can be reached.
You Should Read All Of The Information.
Web request an employee's claim for workers' compensation benefits form from your supervisor (it's also known as a dwc 1 form). Employer's report of occupational injury or illness: Keep this sheet and all other papers for your records. If you are injured or become ill, either physically or mentally, because of your job, including injuries resulting from a workplace crime, you may be entitled to workers’ compensation benefits.