Generali Patient Authorization Form
Generali Patient Authorization Form - Web patient authorization form patient authorization form name of patient: A patient authorization form is a document authorizing a healthcare provider to share a patient’s medical history with a third party. Provider to complete sections c and d. Web patient authorization for release of medical information to third party please print patient information location(s) of service (check. Web edit generali patient authorization form. Web generali is committed to providing prompt, fair and equitable claims service. Web instructions for completing hrsa authorization for use or disclosure of health information type or print legibly in all fields using dark. Web patient authorization form generali. Travel insurance claim doctors and/or medical. Web up to $40 cash back 01 to fill out the patient authorization form for generali, you will need the following information and documents:
Start here to file your travel insurance claim online or contact our claims group. Check out how easy it is to complete and esign documents online using fillable templates and a powerful editor. Web generali is committed to providing prompt, fair and equitable claims service. Web instructions for completing hrsa authorization for use or disclosure of health information type or print legibly in all fields using dark. Easily fill out pdf blank, edit, and sign them. Ease by signing below, i authorize my. Quickly add and highlight text, insert pictures, checkmarks, and signs, drop new fillable fields, and rearrange or remove pages from. Web patient authorization for release of medical information to third party please print patient information location(s) of service (check. Member/provider to complete sections a and b. Web patient authorization form generali.
Web patient authorization for release of medical information to third party please print patient information location(s) of service (check. Web instructions for completing hrsa authorization for use or disclosure of health information type or print legibly in all fields using dark. Web patient authorization form patient authorization form name of patient: Web what is the patient authorization form? Provider to complete sections c and d. Quickly add and highlight text, insert pictures, checkmarks, and signs, drop new fillable fields, and rearrange or remove pages from. Easily fill out pdf blank, edit, and sign them. Ease by signing below, i authorize my. Web instructions for filing a medical claim please type or print and include all requested information a separate claim form must be completed for each family member. Start here to file your travel insurance claim online or contact our claims group.
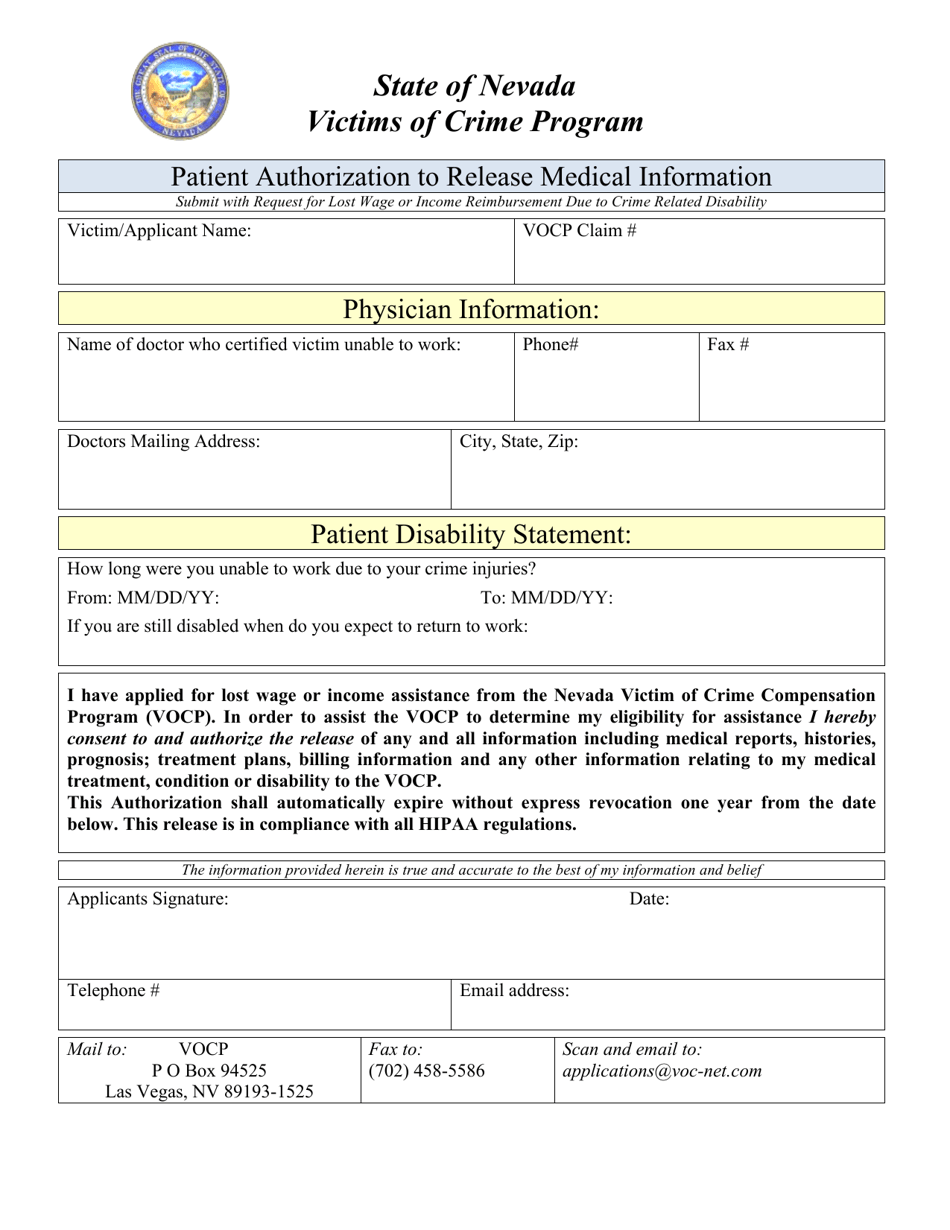
Nevada Patient Authorization to Release Medical Information Download
Web generali.rs medical treatment authorization form patient / insured details medical institution details to be filled out by the insured: Provider to complete sections c and d. Travel insurance claim doctors and/or medical. Web instructions for filing a medical claim please type or print and include all requested information a separate claim form must be completed for each family member..

Printable Patient Authorization Form Template Word
Web instructions for completing hrsa authorization for use or disclosure of health information type or print legibly in all fields using dark. Web patient authorization form generali. Member/provider to complete sections a and b. Start here to file your travel insurance claim online or contact our claims group. Web what is the patient authorization form?
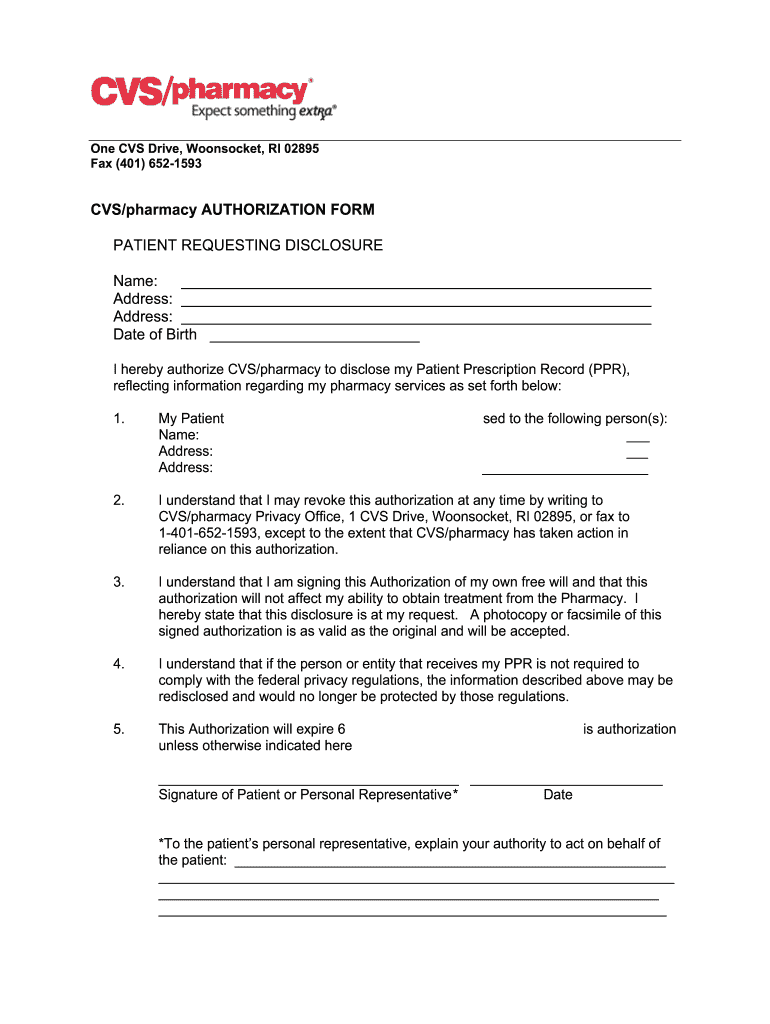
CVS/pharmacy Patient Authorization Form Fill and Sign Printable
Quickly add and highlight text, insert pictures, checkmarks, and signs, drop new fillable fields, and rearrange or remove pages from. Web edit generali patient authorization form. Easily fill out pdf blank, edit, and sign them. Web generali.rs medical treatment authorization form patient / insured details medical institution details to be filled out by the insured: A patient authorization form is.
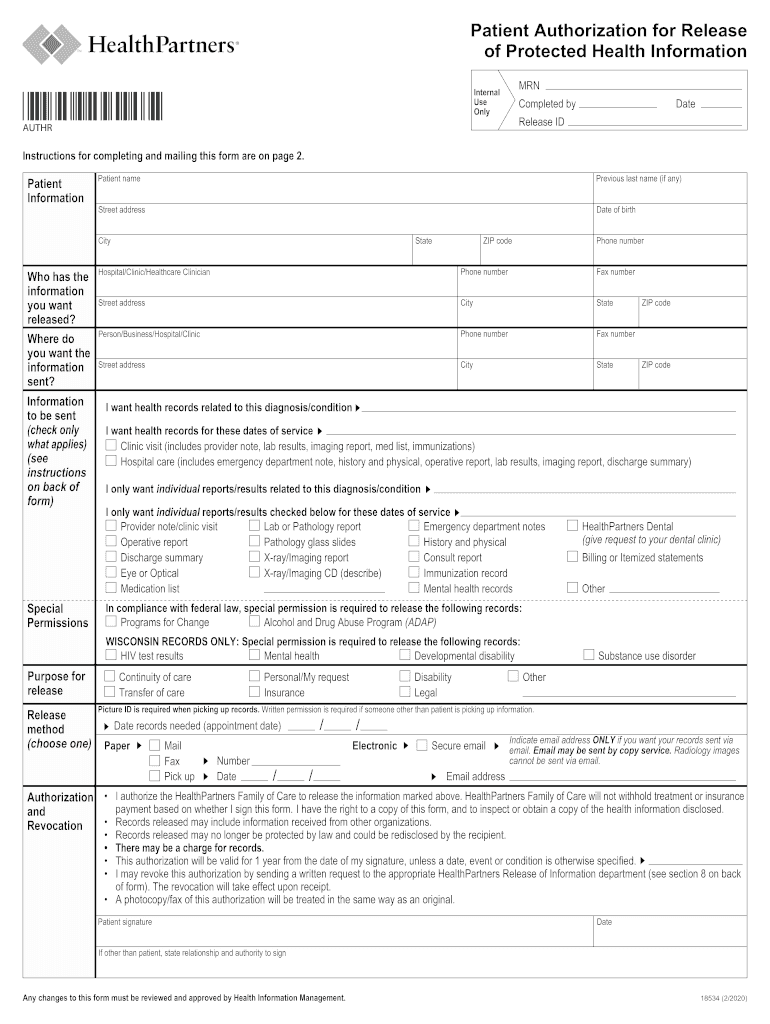
Healthpartners Release Of Information Fill Out and Sign Printable PDF
Easily fill out pdf blank, edit, and sign them. Check out how easy it is to complete and esign documents online using fillable templates and a powerful editor. Web get patient authorization form generali get form show details on required for all hospital admissions, outpatient surgery, rehab treatment, chemotherapy, radiation. Web generali.rs medical treatment authorization form patient / insured details.
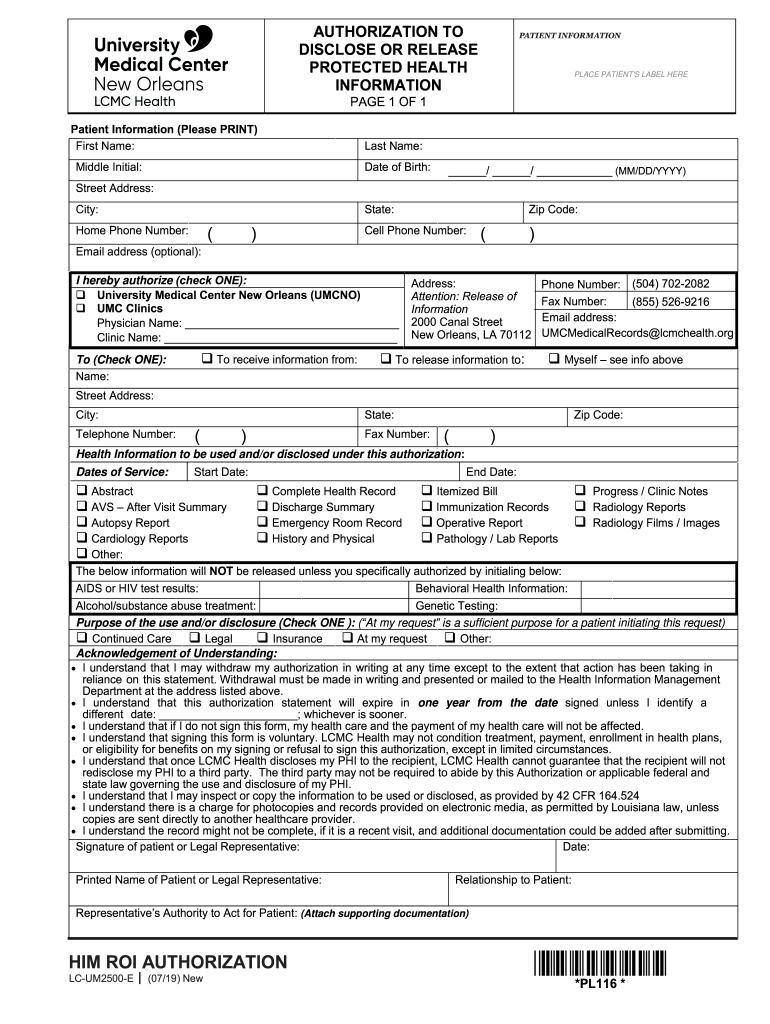
AUTHORIZATION to PATIENTT INFORMATION Fill Out and Sign Printable PDF
Web a patient authorization form must be obtained from the patient for phi to be shared for any reasons other than tpo and the other exemptions. Web get patient authorization form generali get form show details on required for all hospital admissions, outpatient surgery, rehab treatment, chemotherapy, radiation. Member/provider to complete sections a and b. Web patient authorization for release.
Patient Authorization For The Disclosure Of Protected Health
Provider to complete sections c and d. Web what is the patient authorization form? Web instructions for filing a medical claim please type or print and include all requested information a separate claim form must be completed for each family member. Web generali is committed to providing prompt, fair and equitable claims service. Web a patient authorization form must be.
Authorization For Release Of Protected Health Information Template
Provider to complete sections c and d. Travel insurance claim doctors and/or medical. The insured employee should fill out part i, either for himself or his. Quickly add and highlight text, insert pictures, checkmarks, and signs, drop new fillable fields, and rearrange or remove pages from. Web instructions for completing hrsa authorization for use or disclosure of health information type.
Patient Authorization For Disclosure Of Protected Health Information
Check out how easy it is to complete and esign documents online using fillable templates and a powerful editor. Start here to file your travel insurance claim online or contact our claims group. Web generali.rs medical treatment authorization form patient / insured details medical institution details to be filled out by the insured: Web a patient authorization form must be.
FREE 13+ Prior Authorization Forms in PDF MS Word
Travel insurance claim doctors and/or medical. Quickly add and highlight text, insert pictures, checkmarks, and signs, drop new fillable fields, and rearrange or remove pages from. Ease by signing below, i authorize my. Web patient authorization form generali. Provider to complete sections c and d.
FREE 35+ Sample Authorization Forms in PDF
Web a patient authorization form must be obtained from the patient for phi to be shared for any reasons other than tpo and the other exemptions. Web generali is committed to providing prompt, fair and equitable claims service. Travel insurance claim doctors and/or medical. Web edit generali patient authorization form. Web generali.rs medical treatment authorization form patient / insured details.
Member/Provider To Complete Sections A And B.
Web edit generali patient authorization form. Travel insurance claim doctors and/or medical. Web generali is committed to providing prompt, fair and equitable claims service. Web patient authorization form patient authorization form name of patient:
Web Patient Authorization Form Please Sign Patient Authorization To Use/Disclose Health Information:
Provider to complete sections c and d. Save or instantly send your ready documents. Web patient authorization for release of medical information to third party please print patient information location(s) of service (check. Web up to $40 cash back 01 to fill out the patient authorization form for generali, you will need the following information and documents:
Web What Is The Patient Authorization Form?
A patient authorization form is a document authorizing a healthcare provider to share a patient’s medical history with a third party. Start here to file your travel insurance claim online or contact our claims group. Ease by signing below, i authorize my. Easily fill out pdf blank, edit, and sign them.
Check Out How Easy It Is To Complete And Esign Documents Online Using Fillable Templates And A Powerful Editor.
Web generali.rs medical treatment authorization form patient / insured details medical institution details to be filled out by the insured: Quickly add and highlight text, insert pictures, checkmarks, and signs, drop new fillable fields, and rearrange or remove pages from. Web a patient authorization form must be obtained from the patient for phi to be shared for any reasons other than tpo and the other exemptions. Web get patient authorization form generali get form show details on required for all hospital admissions, outpatient surgery, rehab treatment, chemotherapy, radiation.