Hcfa 1500 Form Pdf
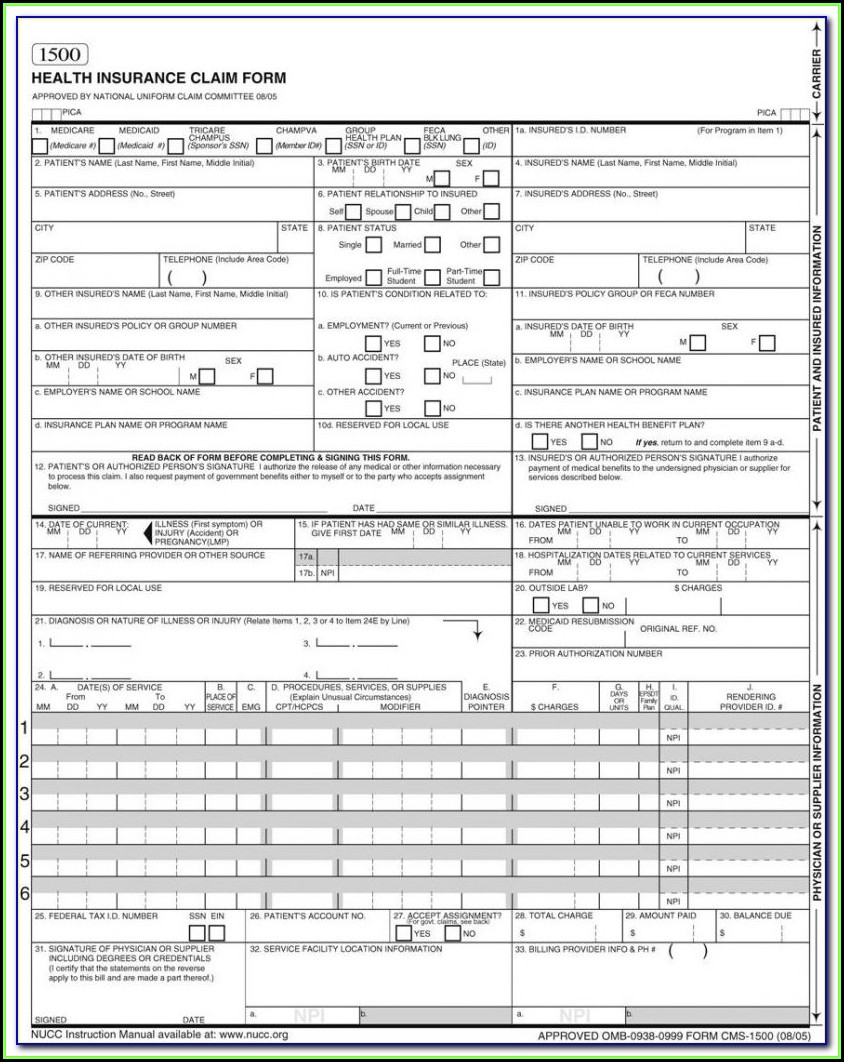
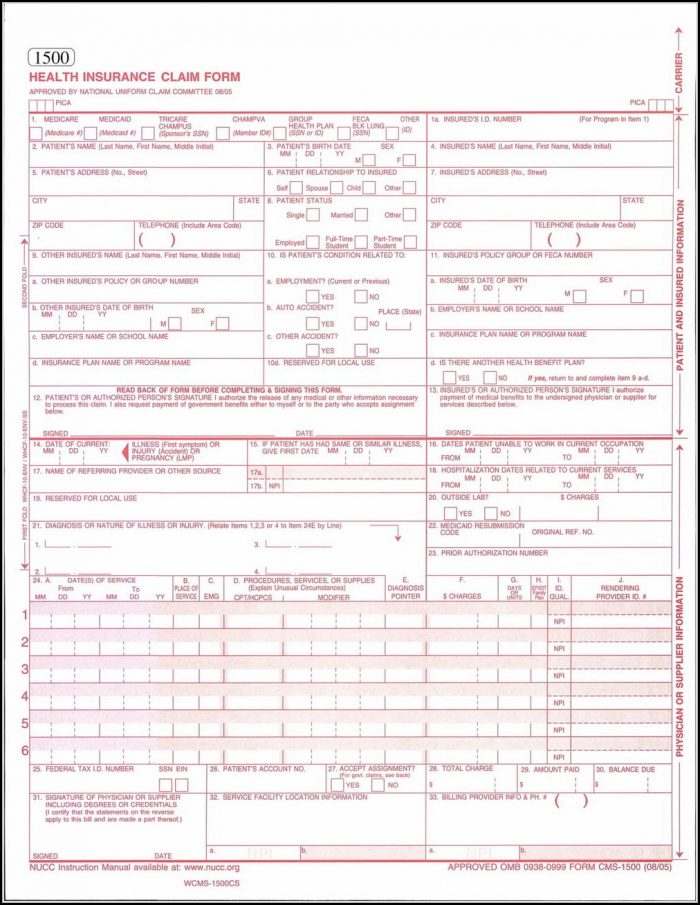
Hcfa 1500 Form Pdf - Insured’s address (no., street) city state zip code telephone (include area code) 11. Number (for program in item 1) 4. It is used for health care claims. Web cms 1500 dynamic list information. When you receive your explanation of medicare benefits papers, attach copies to your hcfa 1500 claim forms. Insured’s name (last name, first name, middle initial) 7. Read the instructions and tips below first. This could be through medicare, champus, group health care, or other forms of insurance. Sign up to get the latest information about your choice of cms topics. Any one who misrepresents or falsifies essential information to receive payment from federal funds requested by this form may upon conviction be subject to fine and imprisonment under applicable federal laws.
Any one who misrepresents or falsifies essential information to receive payment from federal funds requested by this form may upon conviction be subject to fine and imprisonment under applicable federal laws. Number (for program in item 1) 4. We are authorized by hcfa, champus and owcp to ask you for. Sign up to get the latest information about your choice of cms topics. Web hcfa 1500 form | pdf 0 ratings 74 views 1 page hcfa 1500 form uploaded by jeff nakrow copyright: Read the instructions and tips below first. Because this form is used by various government and private health programs, see separate instructions issued by. This could be through medicare, champus, group health care, or other forms of insurance. Please mail them to the name and address listed here. This document is intended to be a guide for completing the 1500 claim form and not definitive instructions for this purpose.
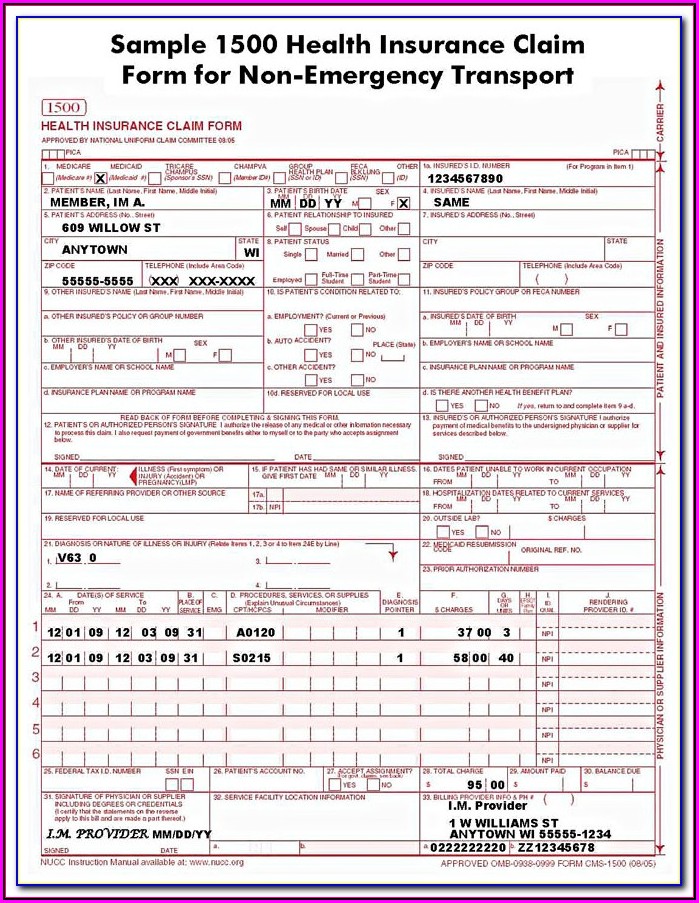
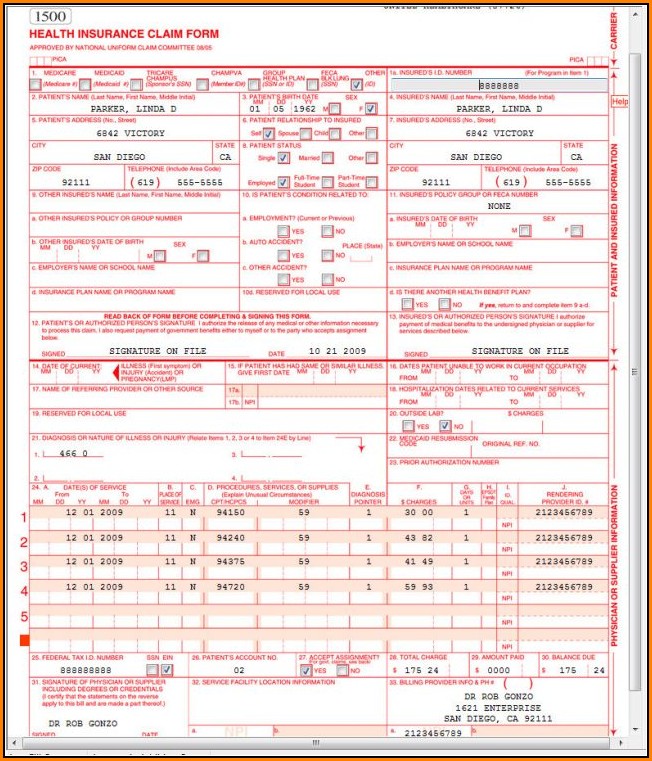
It is used to submit a bill or charge for health insurance coverage. Download free cms 1500 claim form fillable template. This document is intended to be a guide for completing the 1500 claim form and not definitive instructions for this purpose. Sign up to get the latest information about your choice of cms topics. Any one who misrepresents or falsifies essential information to receive payment from federal funds requested by this form may upon conviction be subject to fine and imprisonment under applicable federal laws. When you receive your explanation of medicare benefits papers, attach copies to your hcfa 1500 claim forms. Insured’s address (no., street) city state zip code telephone (include area code) 11. You can decide how often to. Please mail them to the name and address listed here. The current version of the original manual from the national uniform claim comettee of how to complete the cms1500 claim form.
Form Hcfa 1500 Form Resume Examples 4x2v1DQV5l
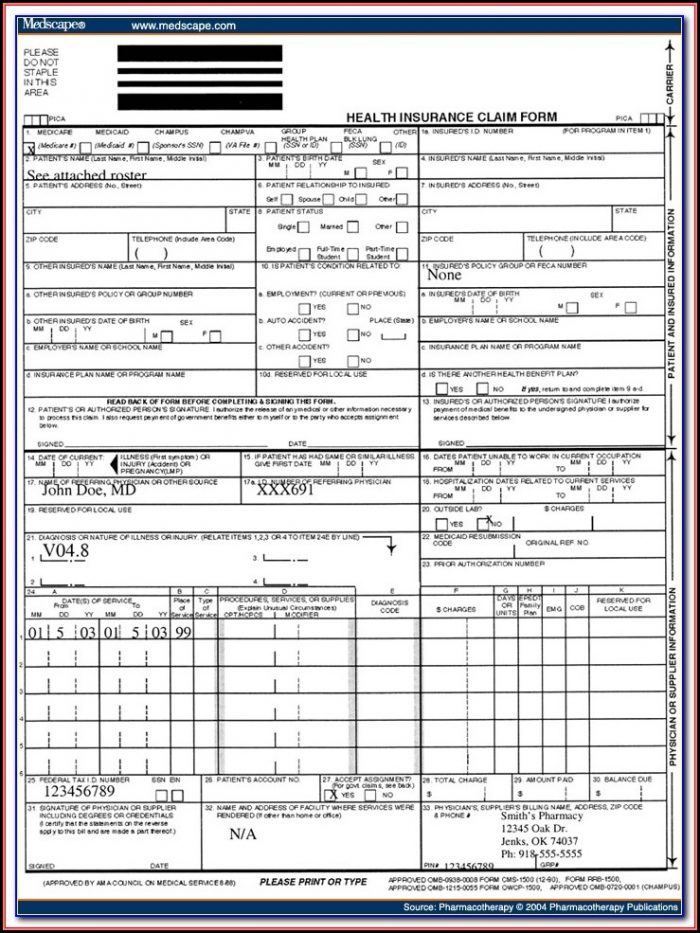
A hcfa 1500 form is used by the health care financing administration. Insured’s name (last name, first name, middle initial) 7. Insured’s policy group or feca number a. You can decide how often to. Download free cms 1500 claim form fillable template.
Hcfa 1500 Form Pdf Fillable Form Resume Examples a6Yn87R2Bg
Any one who misrepresents or falsifies essential information to receive payment from federal funds requested by this form may upon conviction be subject to fine and imprisonment under applicable federal laws. Because this form is used by various government and private health programs, see separate instructions issued by. When you receive your explanation of medicare benefits papers, attach copies to.

Hcfa 1500 Form Pdf Form Resume Examples 46V3RQvK7b
Web hcfa 1500 form | pdf 0 ratings 74 views 1 page hcfa 1500 form uploaded by jeff nakrow copyright: This could be through medicare, champus, group health care, or other forms of insurance. We are authorized by hcfa, champus and owcp to ask you for. When you receive your explanation of medicare benefits papers, attach copies to your hcfa.
Hcfa 1500 Forms Free Download Form Resume Examples Or85MMO8Wz
Any one who misrepresents or falsifies essential information to receive payment from federal funds requested by this form may upon conviction be subject to fine and imprisonment under applicable federal laws. Please mail them to the name and address listed here. Web no part b medicare benefits may be paid unless this form is received as required by existing law.
Hcfa 1500 Forms Free Download Form Resume Examples Or85MMO8Wz
It is used for health care claims. This could be through medicare, champus, group health care, or other forms of insurance. Insured’s policy group or feca number a. The current version of the original manual from the national uniform claim comettee of how to complete the cms1500 claim form. Web the 1500 health insurance claim form (1500 claim form) is.
Hcfa 1500 Form Instructions Form Resume Examples mGM9Oo39DL
We are authorized by hcfa, champus and owcp to ask you for. You can decide how often to. Sign up to get the latest information about your choice of cms topics. The nucc has developed this general instructions document for completing the 1500claim form. Insured’s address (no., street) city state zip code telephone (include area code) 11.
Hcfa 1500 Form Download Pdf Form Resume Examples xz20pPEZ2q
Download free cms 1500 claim form fillable template. Insured’s name (last name, first name, middle initial) 7. The current version of the original manual from the national uniform claim comettee of how to complete the cms1500 claim form. Read the instructions and tips below first. Any one who misrepresents or falsifies essential information to receive payment from federal funds requested.
Hcfa 1500 Claim Form Template Download Form Resume Examples 1ZV8ne393X
Web no part b medicare benefits may be paid unless this form is received as required by existing law and regulations (42 cfr 424.32). Web hcfa 1500 form | pdf 0 ratings 74 views 1 page hcfa 1500 form uploaded by jeff nakrow copyright: You can decide how often to. The nucc has developed this general instructions document for completing.
Download Fillable HCFA 1500 Claim Form PDF RTF Word
The current version of the original manual from the national uniform claim comettee of how to complete the cms1500 claim form. This could be through medicare, champus, group health care, or other forms of insurance. This document is intended to be a guide for completing the 1500 claim form and not definitive instructions for this purpose. We are authorized by.
Cms Hcfa 1500 Form Pdf Form Resume Examples EpDLyEE5xR
The current version of the original manual from the national uniform claim comettee of how to complete the cms1500 claim form. It is used for health care claims. You can decide how often to. Because this form is used by various government and private health programs, see separate instructions issued by. Sign up to get the latest information about your.
It Is Used To Submit A Bill Or Charge For Health Insurance Coverage.
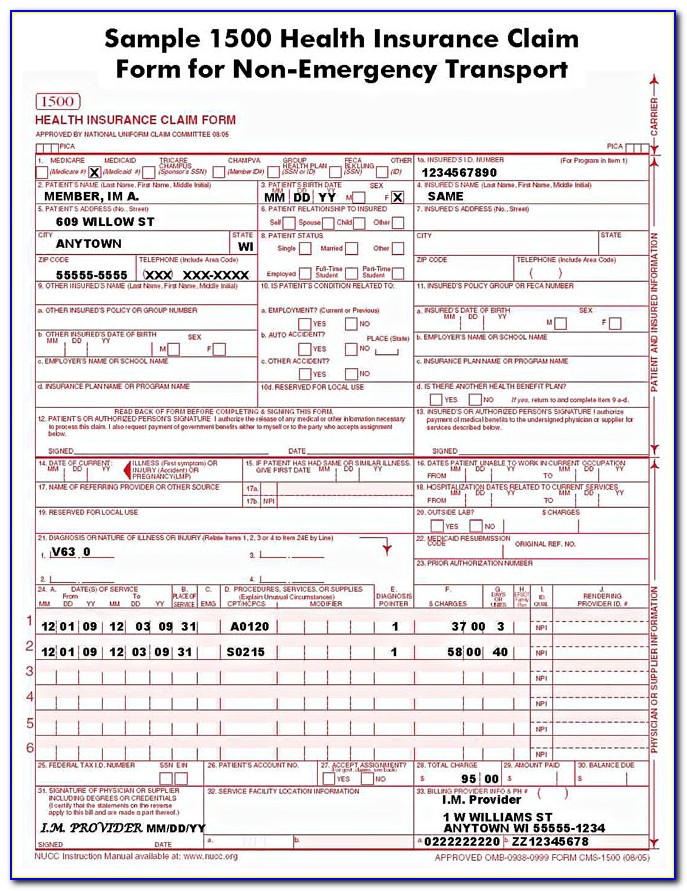
The nucc has developed this general instructions document for completing the 1500claim form. Web the 1500 health insurance claim form (1500 claim form) is in the public domain. The current version of the original manual from the national uniform claim comettee of how to complete the cms1500 claim form. A hcfa 1500 form is used by the health care financing administration.
Web Cms 1500 Dynamic List Information.
Any one who misrepresents or falsifies essential information to receive payment from federal funds requested by this form may upon conviction be subject to fine and imprisonment under applicable federal laws. Because this form is used by various government and private health programs, see separate instructions issued by. Web hcfa 1500 form | pdf 0 ratings 74 views 1 page hcfa 1500 form uploaded by jeff nakrow copyright: Sign up to get the latest information about your choice of cms topics.
Please Mail Them To The Name And Address Listed Here.
It is used for health care claims. You can decide how often to. Insured’s address (no., street) city state zip code telephone (include area code) 11. This could be through medicare, champus, group health care, or other forms of insurance.
When You Receive Your Explanation Of Medicare Benefits Papers, Attach Copies To Your Hcfa 1500 Claim Forms.
Insured’s policy group or feca number a. Insured’s name (last name, first name, middle initial) 7. Number (for program in item 1) 4. This document is intended to be a guide for completing the 1500 claim form and not definitive instructions for this purpose.