Insurance Intake Form
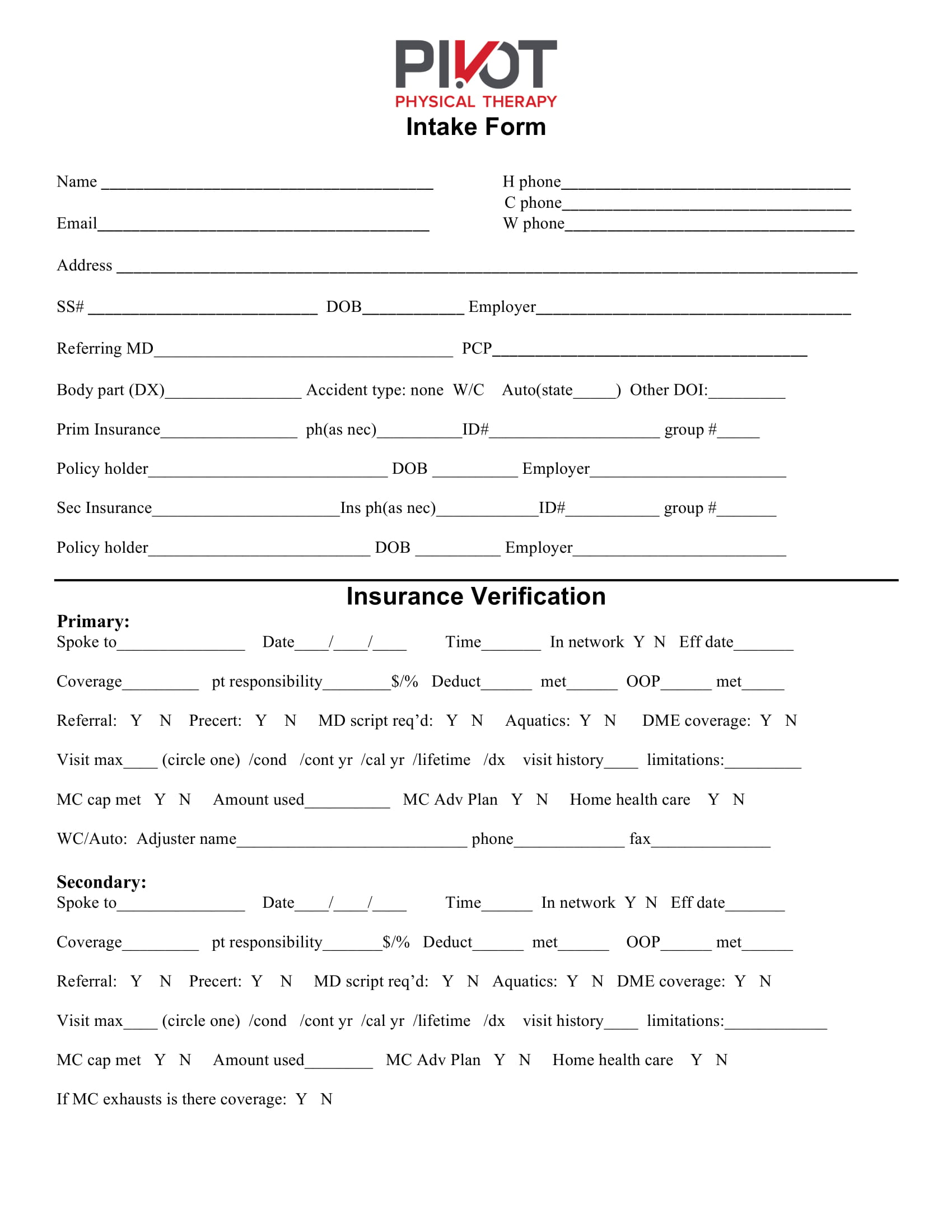
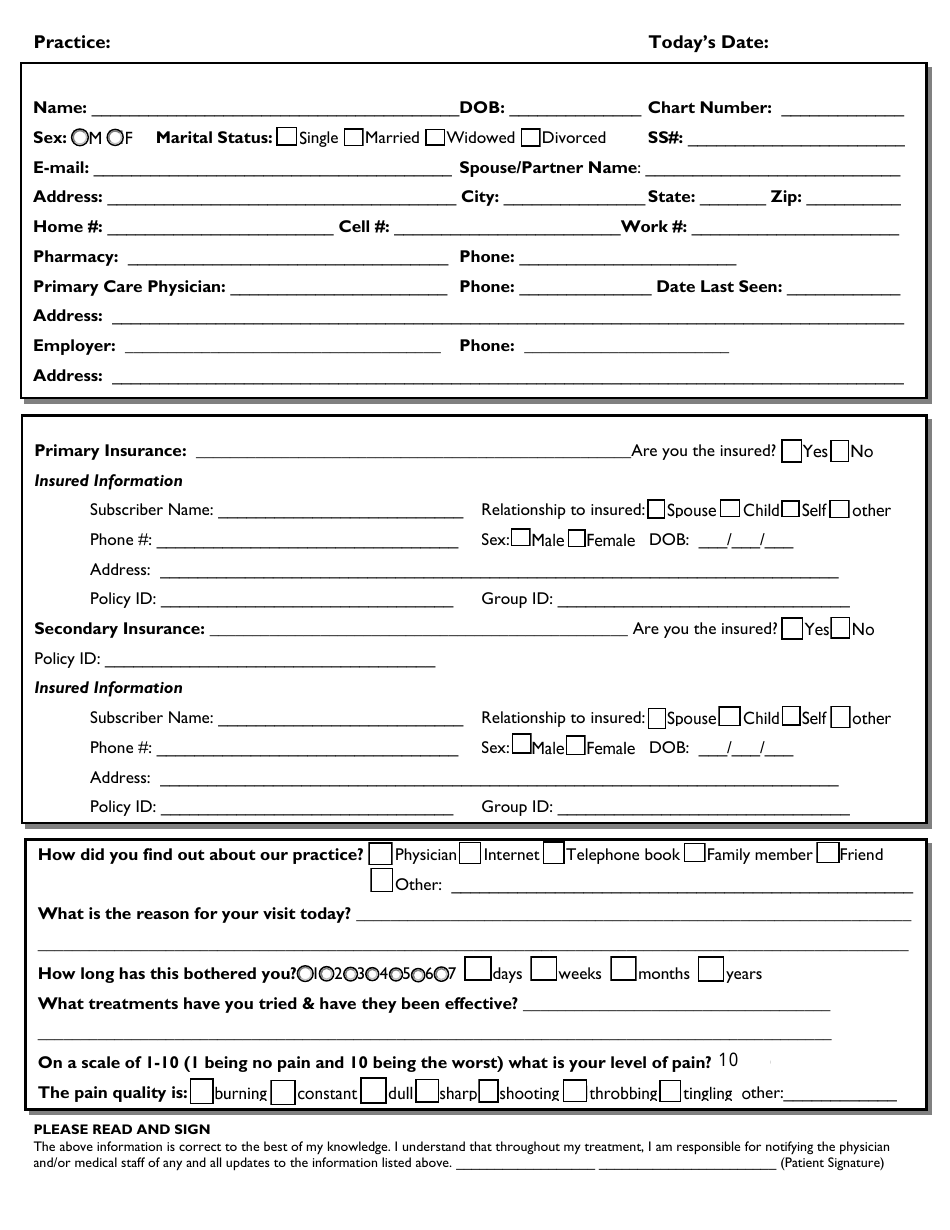
Insurance Intake Form - Web our intake forms are designed to provide you with an easy way to submit a case to our office for review. Web included on this page, you’ll find a legal client intake form, a tax client intake form, a patient intake form, a real estate client intake form, a marketing client intake form, and more. This information will be your basis for deciding the best course of action and devising a perfect strategy on what is to be offered to the client. Web insurance intake form 1. Also, please take a picture of your insurance card and text it to our office line at: Patient's name * first last 2. Please provide us with a brief description of the type of services you are inquiring about * 4. Web 42 printable client intake forms (free templates) a client intake form is a questionnaire that used for the purpose of gathering information that you need from a client. Web guidelines for practice success | managing patients | patient intake request the necessary insurance data and a photo identification when you provide the patient with the standard new patient forms, typically the health history form, a declaration of the practice's payment policy, the health insurance portability and accountability act of 1996. Patients date of birth * mo/dd/year 5.
Also, please take a picture of your insurance card and text it to our office line at: Please provide us with a brief description of the type of services you are inquiring about * 4. This information will be your basis for deciding the best course of action and devising a perfect strategy on what is to be offered to the client. Web guidelines for practice success | managing patients | patient intake request the necessary insurance data and a photo identification when you provide the patient with the standard new patient forms, typically the health history form, a declaration of the practice's payment policy, the health insurance portability and accountability act of 1996. Parent/guardian name if patient is a minor * first last 3. Web insurance intake form please fill in the form click here to review and download.pdfs of the billing service recipient bill of rights and responsibilities, dme pos supplier standards, release of information, notice of privacy practices and billing service description Patients date of birth * mo/dd/year 5. Type a minimum of three characters then press up or down on the keyboard to navigate the autocompleted search results Gender * male female other 6. Plus, get tips on creating a client intake form.
Patient's name * first last 2. Web online intake forms and practice management software from electronic forms and appointment scheduling to insurance billing and secure patient portals, everything you need to manage your entire practice with ease. Web manage patient information in your medical practice with a free health insurance intake form — simply customize the form to match your practice and your patients, and it’s ready to use. Patients date of birth * mo/dd/year 5. Web our intake forms are designed to provide you with an easy way to submit a case to our office for review. This information will be your basis for deciding the best course of action and devising a perfect strategy on what is to be offered to the client. Plus, get tips on creating a client intake form. Type a minimum of three characters then press up or down on the keyboard to navigate the autocompleted search results Please provide us with a brief description of the type of services you are inquiring about * 4. Also, please take a picture of your insurance card and text it to our office line at:

Pin on Example Printable Form Templates Design
Web our intake forms are designed to provide you with an easy way to submit a case to our office for review. Type a minimum of three characters then press up or down on the keyboard to navigate the autocompleted search results Patient's name * first last 2. This information will be your basis for deciding the best course of.

√ 24 Counseling Intake forms Templates in 2020 Templates, Counseling
Web 42 printable client intake forms (free templates) a client intake form is a questionnaire that used for the purpose of gathering information that you need from a client. Web included on this page, you’ll find a legal client intake form, a tax client intake form, a patient intake form, a real estate client intake form, a marketing client intake.
Insurance Verification Form Pdf
Please provide us with a brief description of the type of services you are inquiring about * 4. Web hello and welcome to bcs llc servics! This information will be your basis for deciding the best course of action and devising a perfect strategy on what is to be offered to the client. Web guidelines for practice success | managing.
New Patient Intake Form Download Fillable PDF Templateroller
Please fill out the contact form below so that we may began composing your charts. Web insurance intake form 1. Plus, get tips on creating a client intake form. We're happy you chose us. Web online intake forms and practice management software from electronic forms and appointment scheduling to insurance billing and secure patient portals, everything you need to manage.

Mid America Rehab Patient Intake Form Fill and Sign Printable
We're happy you chose us. Web insurance intake form please fill in the form click here to review and download.pdfs of the billing service recipient bill of rights and responsibilities, dme pos supplier standards, release of information, notice of privacy practices and billing service description Web guidelines for practice success | managing patients | patient intake request the necessary insurance.
Patient Intake Form
Web hello and welcome to bcs llc servics! Web guidelines for practice success | managing patients | patient intake request the necessary insurance data and a photo identification when you provide the patient with the standard new patient forms, typically the health history form, a declaration of the practice's payment policy, the health insurance portability and accountability act of 1996..
Customer Vehicle Intake Form page 2 Digital Download Etsy
Web insurance intake form please fill in the form click here to review and download.pdfs of the billing service recipient bill of rights and responsibilities, dme pos supplier standards, release of information, notice of privacy practices and billing service description Web manage patient information in your medical practice with a free health insurance intake form — simply customize the form.
Horizon View Health Patient Intake Form Fill and Sign Printable
Plus, get tips on creating a client intake form. Please provide us with a brief description of the type of services you are inquiring about * 4. This information will be your basis for deciding the best course of action and devising a perfect strategy on what is to be offered to the client. Patient's name * first last 2..
Client/Patient Intake Form Download Printable PDF Templateroller
Parent/guardian name if patient is a minor * first last 3. You can even add your logo and change the color scheme, fonts, and backgrounds to make it your own! Web manage patient information in your medical practice with a free health insurance intake form — simply customize the form to match your practice and your patients, and it’s ready.

Template Insurance Proposal Form INSURANCE DAY
Web insurance intake form 1. Please take a picture of the front and back. Web insurance intake form please fill in the form click here to review and download.pdfs of the billing service recipient bill of rights and responsibilities, dme pos supplier standards, release of information, notice of privacy practices and billing service description Web manage patient information in your.
Web Hello And Welcome To Bcs Llc Servics!
Web online intake forms and practice management software from electronic forms and appointment scheduling to insurance billing and secure patient portals, everything you need to manage your entire practice with ease. Gender * male female other 6. Web insurance intake form 1. Parent/guardian name if patient is a minor * first last 3.
Street , City, State, Zip * 7.
We're happy you chose us. Web included on this page, you’ll find a legal client intake form, a tax client intake form, a patient intake form, a real estate client intake form, a marketing client intake form, and more. Please take a picture of the front and back. Web insurance intake form please fill in the form click here to review and download.pdfs of the billing service recipient bill of rights and responsibilities, dme pos supplier standards, release of information, notice of privacy practices and billing service description
Web Guidelines For Practice Success | Managing Patients | Patient Intake Request The Necessary Insurance Data And A Photo Identification When You Provide The Patient With The Standard New Patient Forms, Typically The Health History Form, A Declaration Of The Practice's Payment Policy, The Health Insurance Portability And Accountability Act Of 1996.
Please provide us with a brief description of the type of services you are inquiring about * 4. Also, please take a picture of your insurance card and text it to our office line at: Web manage patient information in your medical practice with a free health insurance intake form — simply customize the form to match your practice and your patients, and it’s ready to use. Plus, get tips on creating a client intake form.
Patients Date Of Birth * Mo/Dd/Year 5.
Type a minimum of three characters then press up or down on the keyboard to navigate the autocompleted search results You can even add your logo and change the color scheme, fonts, and backgrounds to make it your own! Please fill out the contact form below so that we may began composing your charts. Patient's name * first last 2.