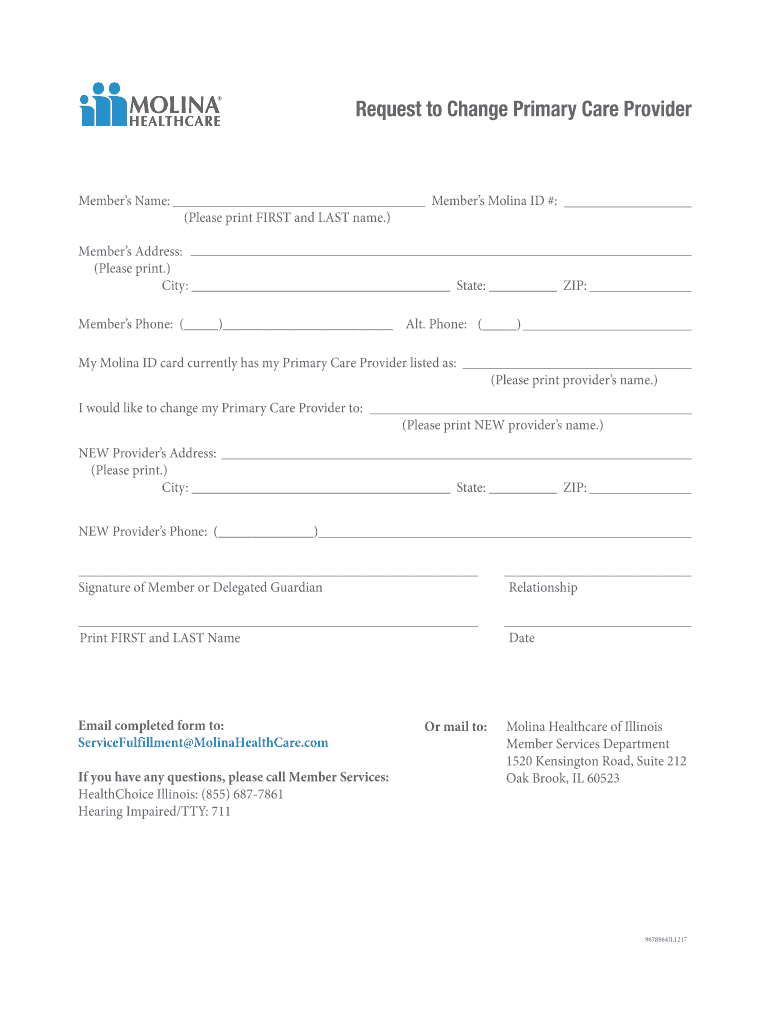
Molina Pcp Change Form
Molina Pcp Change Form - Request to change primary care provider ☐ new member—1st time selection ☐ provider location ☐ already. Easily fill out pdf blank, edit, and sign her. Easily filling out pdf blank, print, and signing them. Use get form or simply click on the template preview to open it in the editor. Start completing the fillable fields. Web the form, please call the number on the back of the id card. Web i would like to change my primary care provider to: Please print new provider’s name new provider’s address: Web molina request change form. Web how can i help a member change their assigned pcp?
Web complete molina pcp change form online with us legal forms. Web 4.8 satisfied 145 votes how to fill out and sign molina healthcare pcp change form online? Get everything done in minutes. Web change and esign molina healthcare pcp form and ensure excellent communication at any stage of the form preparation process with signnow. Sign it in a few clicks draw your. Web the form, please call the number on the back of the id card. Check out how easy it is to complete plus esign records internet using fillable templates and a powerful editor. Web first of the current month if the member is new to molina healthcare this month, has not received services from any other provider and the change request form. Web you can also select or change your pcp online: Web molina request change form.
Web i would like to change my primary care provider to: Web you can also select or change your pcp online: Get everything done in minutes. Sign it in a few clicks draw your. Web the form, please call the number on the back of the id card. Be ready to get more create. Request to change primary care provider ☐ new member—1st time selection ☐ provider location ☐ already. Web first of the current month if the member is new to molina healthcare this month, has not received services from any other provider and the change request form. Pcp changes will require 48 hours to. Please print new provider’s name new provider’s address:
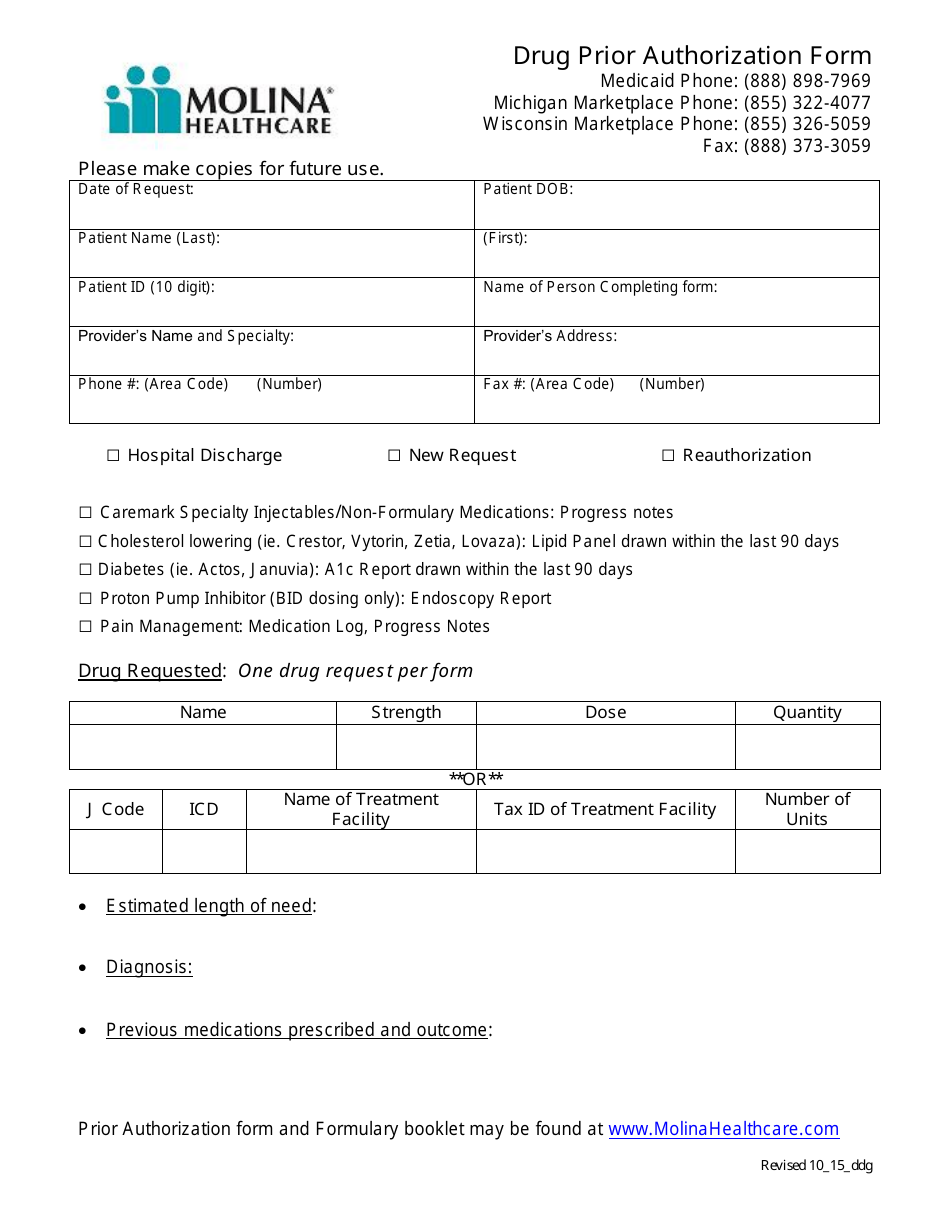
Drug Prior Authorization Form Molina Healthcare Download Printable
Sign it in a few clicks draw your. Get everything done in minutes. Web i would like to change my primary care provider to: Web member pcp change request form member pcp change request form please complete one form per member or household. Please print new provider’s name new provider’s address:

Molina Drug Prior Authorization Fill Online, Printable, Fillable
Sign it in a few clicks draw your. Check out how easy it is to complete plus esign records internet using fillable templates and a powerful editor. Easily fill out pdf blank, edit, and sign them. Web complete molina pcp change form online with us legal forms. We will be unable to process your request unless all fields are completed.

Ambetter Agent Resources Plans And Client Brochures
Web please complete this form if the pcp on your molina healthcare id card is incorrect. Web first of the current month if the member is new to molina healthcare this month, has not received services from any other provider and the change request form. Start completing the fillable fields. Check out how easy it is to complete and esign.

pcp change form Dr. Kashif Anwar, MD
Web molina request change form. Please print new provider’s name new provider’s address: Web would like to change my primary care provider to: Web i would like to change my primary care provider to: We will be unable to process your request unless all fields are completed for each.
Healthcare Request Change Fill Out and Sign Printable PDF Template
Web how can i help a member change their assigned pcp? Web edit your change primary provider form online type text, add images, blackout confidential details, add comments, highlights and more. Easily fill out pdf blank, edit, and sign them. Web would like to change my primary care provider to: Sign it in a few clicks draw your.

MOLINA HEALTHCARE, INC. FORM 8K EX99.1 September 16, 2011
We will be unable to process your request unless all fields are completed for each. Web molina request change form. Check out how easy it is to complete and esign documents online using fillable templates and a powerful editor. Start completing the fillable fields. Please print new provider’s name new provider’s address:

MOLINA HEALTHCARE, INC. FORM 8K EX99.1 January 11, 2011
Easily fill out pdf blank, edit, and sign her. Get everything done in minutes. Web you can also select or change your pcp online: Please print new provider’s name new provider’s address: Be ready to get more create.

2008 Form DD 2876 Fill Online, Printable, Fillable, Blank pdfFiller
Web molina request change form. Please print new provider’s name. Check out how easy it is to complete plus esign records internet using fillable templates and a powerful editor. He or she will be your personal doctor. Web you can also select or change your pcp online:
MOLINA HEALTHCARE, INC. FORM 8K EX99.2 SLIDE PRESENTATION GIVEN
Easily fill out pdf blank, edit, and sign her. Be ready to get more create. Web molina request change form. Sign it in a few clicks draw your. Easily fill out pdf blank, edit, and sign them.
MOLINA HEALTHCARE, INC. FORM 8K EX99.2 SLIDE PRESENTATION GIVEN
Use get form or simply click on the template preview to open it in the editor. Request to change primary care provider ☐ new member—1st time selection ☐ provider location ☐ already. We will be unable to process your request unless all fields are completed for each. Sign it in a few clicks draw your. Web i would like to.
Web Edit Your Change Primary Provider Form Online Type Text, Add Images, Blackout Confidential Details, Add Comments, Highlights And More.
Web 4.8 satisfied 145 votes how to fill out and sign molina healthcare pcp change form online? Use get form or simply click on the template preview to open it in the editor. Web molina request change form. Web change and esign molina healthcare pcp form and ensure excellent communication at any stage of the form preparation process with signnow.
Web Member Pcp Change Request Form Member Pcp Change Request Form Please Complete One Form Per Member Or Household.
Pcp changes will require 48 hours to. Easily filling out pdf blank, print, and signing them. Get everything done in minutes. Web would like to change my primary care provider to:
Start Completing The Fillable Fields.
Web i would like to change my primary care provider to: Web you can also select or change your pcp online: Web marketplace > your pcp marketplace pcp is your personal doctor pcp stands for primary care provider. Request to change primary care provider ☐ new member—1st time selection ☐ provider location ☐ already.
Check Out How Easy It Is To Complete Plus Esign Records Internet Using Fillable Templates And A Powerful Editor.
Please print new provider’s name. Web please complete this form if the pcp on your molina healthcare id card is incorrect. He or she will be your personal doctor. Please print new provider’s name new provider’s address: