Notice Of Privacy Practices Acknowledgement Form Pdf
Notice Of Privacy Practices Acknowledgement Form Pdf - Web by signing this form, you acknowledge that we have provided you with our notice of privacy practices which explains how your health information may be handled in. Web acknowledgement of department of veterans affairs, veterans health administration (vha) notice of privacy practices the signature below only acknowledges receipt of. The purpose of this form is to provide notification to patients and/or sponsors about the personal information that may be collected and how it is intended to be used, and to. Web notice of privacy practices. If the individual or personal representative did not sign above,. The signature below acknowledges receipt of the vha notice of privacy practices only. Department of health and human services 200 independence avenue, s.w. Web privacy policy acknowledgement form i acknowledge that i have received a copy of the privacy policies from the florida department of law enforcement and the. If you decline to provide a signed acknowledgment, med. Web this notice of privacy practices describes how we may use and disclose your protected health information (phi) to carry out treatment, payment or health care.
Web notice of privacy practices template. Web a covered entity must document compliance with the notice requirements, as required by § 164.530(j), by retaining copies of the notices issued by the covered entity and, if. Web acknowledgment of receipt notice of privacy practices i acknowledge that i have received a copy of wellstar health system's notice of privacy practices for. Web notice of privacy practices. Web by signing this form, you acknowledge that we have provided you with our notice of privacy practices which explains how your health information may be handled in. _____ birthdate:_____ the notice of privacy practices. If you decline to provide a signed acknowledgment, med. Web ðï ࡱ á> þÿ ƒ þÿÿÿ. The signature below acknowledges receipt of the vha notice of privacy practices only. Web acknowledgement of department of veterans affairs, veterans health administration (vha) notice of privacy practices the signature below only acknowledges receipt of.
The purpose of this form is to provide notification to patients and/or sponsors about the personal information that may be collected and how it is intended to be used, and to. Web ðï ࡱ á> þÿ ƒ þÿÿÿ. Web notice of privacy practices acknowledgment form name of patient (print): Nc department of health and human services (ncdhhs) form effective date. Web notice of privacy practices the signature below only acknowledges receipt of the vha notice of privacy practices, effective date 30 september 2019. Web individual's behalf, the notice must be given to and acknowledgment obtained form the personal representative. Web by signing this form, you acknowledge that we have provided you with our notice of privacy practices which explains how your health information may be handled in. If you decline to provide a signed acknowledgment, med. The signature below acknowledges receipt of the vha notice of privacy practices only. Web notice of privacy practices acknowledgement & signature form patients name (please print):
Receipt Acknowledgement Of Privacy Practices Templates at
Web individual's behalf, the notice must be given to and acknowledgment obtained form the personal representative. Web by signing this form, you acknowledge that we have provided you with our notice of privacy practices which explains how your health information may be handled in. Web notice of privacy practices acknowledgment form name of patient (print): _____ birthdate:_____ the notice of.
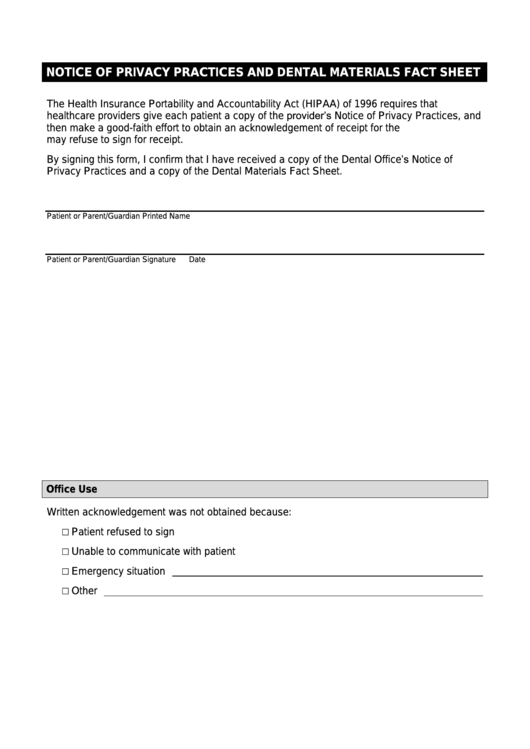
Fillable Notice Of Privacy Practices And Dental Materials Fact Sheet
Web a covered entity must document compliance with the notice requirements, as required by § 164.530(j), by retaining copies of the notices issued by the covered entity and, if. The purpose of this form is to provide notification to patients and/or sponsors about the personal information that may be collected and how it is intended to be used, and to..
FREE 5+ Sample Privacy Notice Forms in MS Word PDF
If you decline to provide a signed acknowledgment, med. If the individual or personal representative did not sign above,. The signature below acknowledges receipt of the vha notice of privacy practices only. Web notice of privacy practices. Web a covered entity must document compliance with the notice requirements, as required by § 164.530(j), by retaining copies of the notices issued.
Hipaa Notice Of Privacy Practices Form Missouri printable pdf download
Web acknowledgment of receipt notice of privacy practices i acknowledge that i have received a copy of wellstar health system's notice of privacy practices for. The purpose of this form is to provide notification to patients and/or sponsors about the personal information that may be collected and how it is intended to be used, and to. Web notice of privacy.

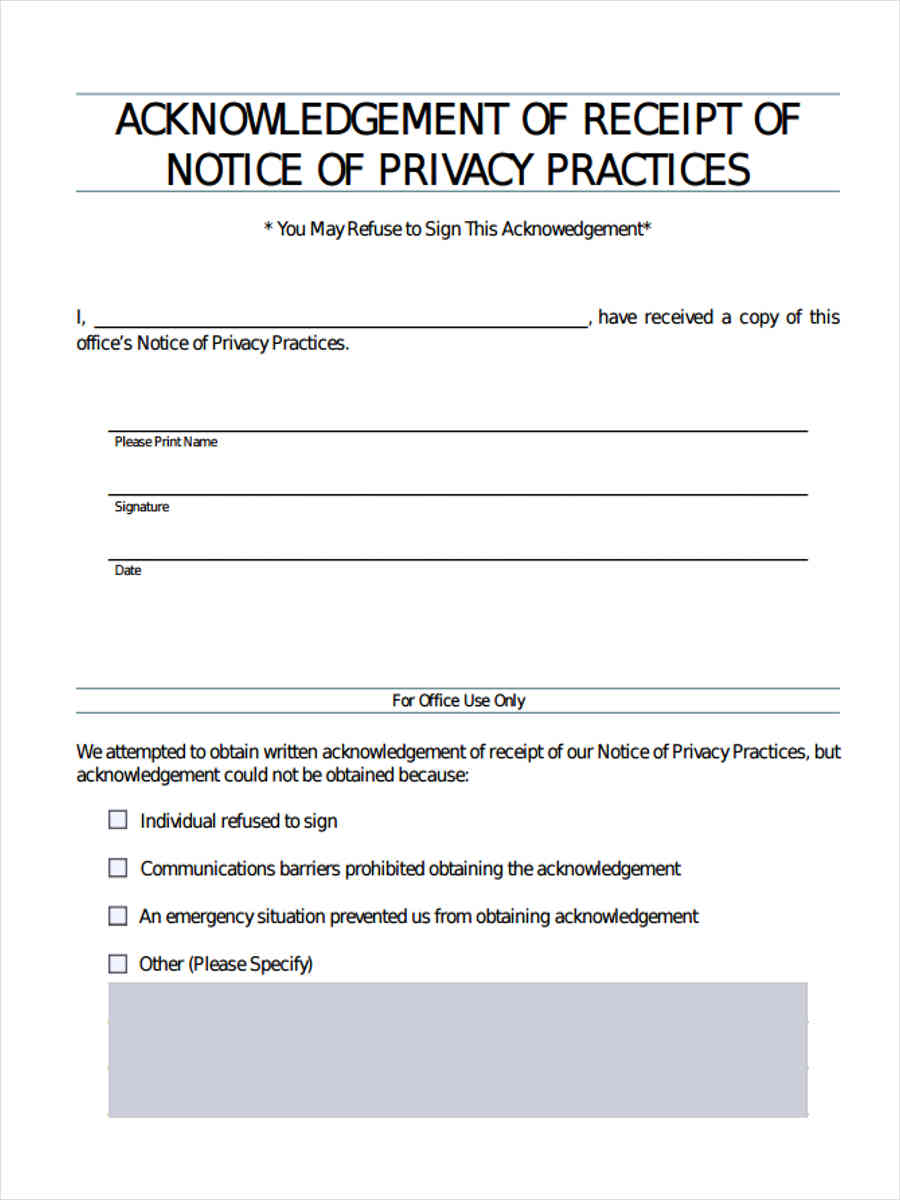
Hipaa Privacy Rule Receipt Of Notice Of Privacy Practices Written
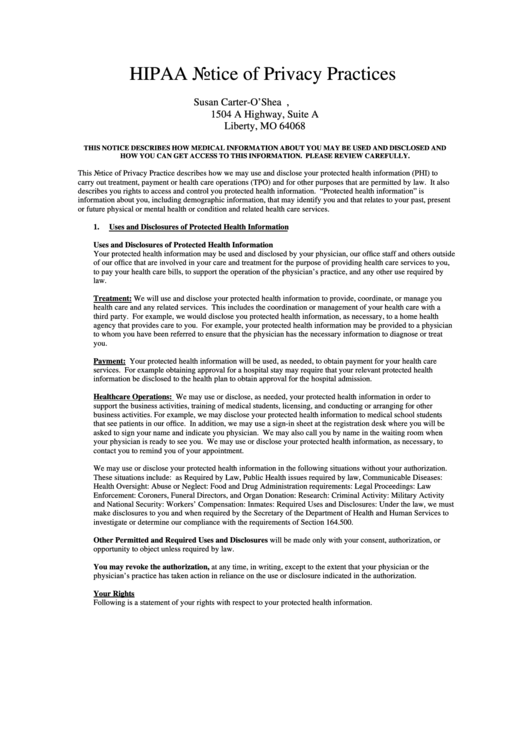
Web this notice of privacy practices describes how we may use and disclose your protected health information (phi) to carry out treatment, payment or health care. Web individual's behalf, the notice must be given to and acknowledgment obtained form the personal representative. The purpose of this form is to provide notification to patients and/or sponsors about the personal information that.

Form HIPPAF2 Download Printable PDF or Fill Online Notice of Privacy
Web notice of privacy practices the signature below only acknowledges receipt of the vha notice of privacy practices, effective date 30 september 2019. _____ birthdate:_____ the notice of privacy practices. Web acknowledgment of receipt notice of privacy practices i acknowledge that i have received a copy of wellstar health system's notice of privacy practices for. Web ðï ࡱ á> þÿ.
Form HipaaF2 Notice Of Privacy Practices Acknowledgment Form
Department of health and human services 200 independence avenue, s.w. If you decline to provide a signed acknowledgment, med. Web notice of privacy practices acknowledgment form name of patient (print): The purpose of this form is to provide notification to patients and/or sponsors about the personal information that may be collected and how it is intended to be used, and.
FREE 7+ Privacy Notice Forms in PDF
Web notice of privacy practices. Web this notice of privacy practices describes how we may use and disclose your protected health information (phi) to carry out treatment, payment or health care. Web privacy policy acknowledgement form i acknowledge that i have received a copy of the privacy policies from the florida department of law enforcement and the. If you decline.
Notice of privacy practices form Fill out & sign online DocHub
Web notice of privacy practices template. Web individual's behalf, the notice must be given to and acknowledgment obtained form the personal representative. If the individual or personal representative did not sign above,. Web by signing this form, you acknowledge that we have provided you with our notice of privacy practices which explains how your health information may be handled in..
Acknowledgement of Receipt of Notice of Privacy Practices
Web notice of privacy practices acknowledgement the u.s. Web by signing this form, you acknowledge that we have provided you with our notice of privacy practices which explains how your health information may be handled in. Web acknowledgment of receipt notice of privacy practices i acknowledge that i have received a copy of wellstar health system's notice of privacy practices.
Web Notice Of Privacy Practices Acknowledgement The U.s.
Nc department of health and human services (ncdhhs) form effective date. Web notice of privacy practices template. Web this notice of privacy practices describes how we may use and disclose your protected health information (phi) to carry out treatment, payment or health care. Web ðï ࡱ á> þÿ ƒ þÿÿÿ.
Web Acknowledgement Of Department Of Veterans Affairs, Veterans Health Administration (Vha) Notice Of Privacy Practices The Signature Below Only Acknowledges Receipt Of.
Web by signing this form, you acknowledge that we have provided you with our notice of privacy practices which explains how your health information may be handled in. Department of health and human services 200 independence avenue, s.w. Web notice of privacy practices acknowledgement & signature form patients name (please print): Web please review the notice of privacy practices and complete this form as an acknowledgment of receipt.
The Purpose Of This Form Is To Provide Notification To Patients And/Or Sponsors About The Personal Information That May Be Collected And How It Is Intended To Be Used, And To.
Web notice of privacy practices acknowledgment form name: If you decline to provide a signed acknowledgment, med. If the individual or personal representative did not sign above,. Web individual's behalf, the notice must be given to and acknowledgment obtained form the personal representative.
_____ Birthdate:_____ The Notice Of Privacy Practices.
Web notice of privacy practices. Web notice of privacy practices the signature below only acknowledges receipt of the vha notice of privacy practices, effective date 30 september 2019. English version (pdf) arabic version (pdf) chinese version (pdf) haitian version (pdf) khmer version (pdf) portuguese version (pdf) russian. Web notice of privacy practices acknowledgment form name of patient (print):