Orthodontic Release Form
Orthodontic Release Form - Once completed, dental clinics can forward this form to other dentists as proof of authorization to release their particulars to the clinic. This information is necessary for the dentist to have the ability to review the previous records. Web the dental records release form is a document that is provided by a dental patient or the parent or guardian of the patient if the patient is a minor, or of proper relations, for the purpose of obtaining dental records from another dentist or dental specialist. Web it is necessary that your records be transferred to assure that the receiving orthodontist is knowledgeable of your orthodontic condition(s), orthodontic treatment goals, the current treatment plan, and related financial arrangements. Web 01 to fill out the early removal of braces, you should first consult with your orthodontist or dentist. Start completing the fillable fields and carefully type in required information. Use get form or simply click on the template preview to open it in the editor. Parent/guardian name first name last name date date signature clear submit To send just this basic information described above please check here ! 02 if you are eligible for early removal of braces, your orthodontist or dentist will provide you with the necessary paperwork or forms to fill out.
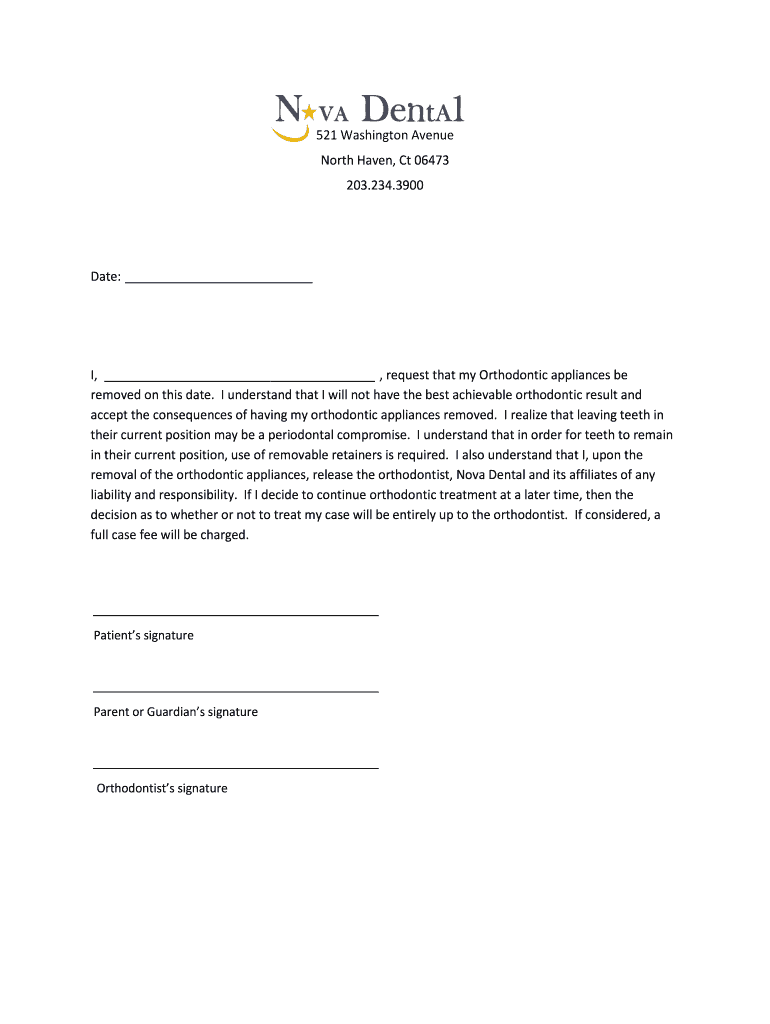
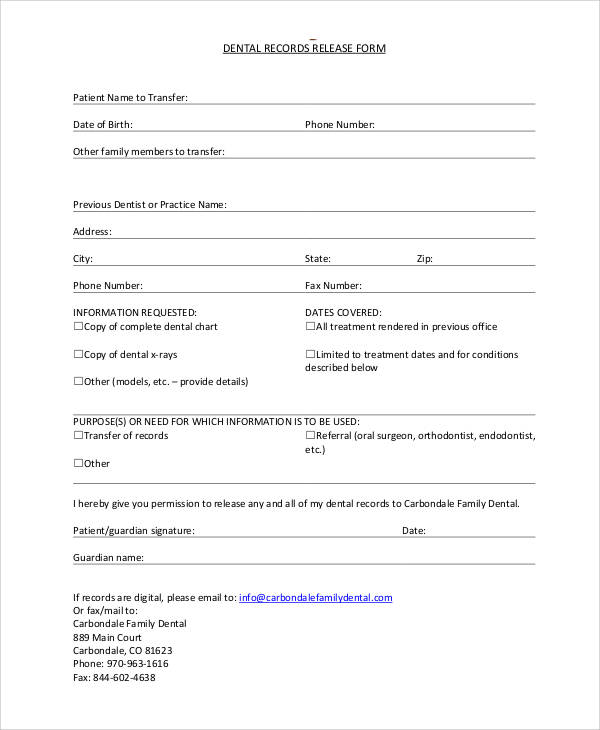
Web it is necessary that your records be transferred to assure that the receiving orthodontist is knowledgeable of your orthodontic condition(s), orthodontic treatment goals, the current treatment plan, and related financial arrangements. Use get form or simply click on the template preview to open it in the editor. To send just this basic information described above please check here ! Web i understand that this is a full waiver and release of any and all claims (i) (my child ___________) or anyone claiming through or on behalf of (me) (my child) may now have or may acquire in the future arising out of the removal of (my) (my child’s) appliances as aforesaid by said doctor, his/her agents or employees. Start completing the fillable fields and carefully type in required information. Web 01 to fill out the early removal of braces, you should first consult with your orthodontist or dentist. Once completed, dental clinics can forward this form to other dentists as proof of authorization to release their particulars to the clinic. 02 if you are eligible for early removal of braces, your orthodontist or dentist will provide you with the necessary paperwork or forms to fill out. To facilitate the transfer of these records, it is necessary that you complete the following: This information is necessary for the dentist to have the ability to review the previous records.
02 if you are eligible for early removal of braces, your orthodontist or dentist will provide you with the necessary paperwork or forms to fill out. Parent/guardian name first name last name date date signature clear submit To facilitate the transfer of these records, it is necessary that you complete the following: Start completing the fillable fields and carefully type in required information. Use the cross or check marks in the top toolbar to select your answers in the list boxes. Web i understand that this is a full waiver and release of any and all claims (i) (my child ___________) or anyone claiming through or on behalf of (me) (my child) may now have or may acquire in the future arising out of the removal of (my) (my child’s) appliances as aforesaid by said doctor, his/her agents or employees. This information is necessary for the dentist to have the ability to review the previous records. Web it is necessary that your records be transferred to assure that the receiving orthodontist is knowledgeable of your orthodontic condition(s), orthodontic treatment goals, the current treatment plan, and related financial arrangements. Once completed, dental clinics can forward this form to other dentists as proof of authorization to release their particulars to the clinic. Web orthodontic records release form patient name first name last name i hereby give my permission to release any/all information pertaining to orthodontic treatment (diagnostic records) and treatment notes for myself/child to the office of dr.
Early Removal Of Braces Consent Form Fill Online, Printable, Fillable
Invisalign® in honolulu and kailua; 02 if you are eligible for early removal of braces, your orthodontist or dentist will provide you with the necessary paperwork or forms to fill out. Parent/guardian name first name last name date date signature clear submit Once completed, dental clinics can forward this form to other dentists as proof of authorization to release their.
FREE 11+ Sample Dental Release Forms in MS Word PDF
Parent/guardian name first name last name date date signature clear submit To send just this basic information described above please check here ! They will assess your specific situation and determine if you are a candidate for early removal. Web i understand that this is a full waiver and release of any and all claims (i) (my child ___________) or.
FREE 11+ Sample Dental Release Forms in MS Word PDF
Use get form or simply click on the template preview to open it in the editor. Once completed, dental clinics can forward this form to other dentists as proof of authorization to release their particulars to the clinic. Invisalign® in honolulu and kailua; To facilitate the transfer of these records, it is necessary that you complete the following: 02 if.

Common Orthodontics Treatments CAPTAIN FLOSS
Use the cross or check marks in the top toolbar to select your answers in the list boxes. Parent/guardian name first name last name date date signature clear submit To send just this basic information described above please check here ! Web it is necessary that your records be transferred to assure that the receiving orthodontist is knowledgeable of your.

Fillable Patient Release Of Dental Records Form printable pdf download
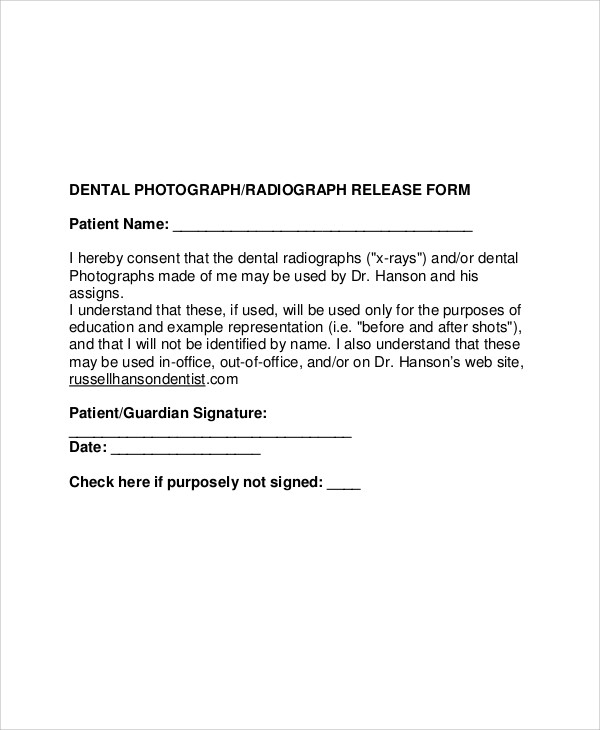
Web orthodontic records release form patient name first name last name i hereby give my permission to release any/all information pertaining to orthodontic treatment (diagnostic records) and treatment notes for myself/child to the office of dr. Web 01 to fill out the early removal of braces, you should first consult with your orthodontist or dentist. Start completing the fillable fields.

Benefits Of Early Orthodontic Treatment And Assessment Viral Rang
They will assess your specific situation and determine if you are a candidate for early removal. Use the cross or check marks in the top toolbar to select your answers in the list boxes. Web it is necessary that your records be transferred to assure that the receiving orthodontist is knowledgeable of your orthodontic condition(s), orthodontic treatment goals, the current.
FREE 53+ Generic Release Forms in PDF
Web orthodontic records release form patient name first name last name i hereby give my permission to release any/all information pertaining to orthodontic treatment (diagnostic records) and treatment notes for myself/child to the office of dr. Once completed, dental clinics can forward this form to other dentists as proof of authorization to release their particulars to the clinic. Web 01.
FREE 11+ Sample Dental Release Forms in MS Word PDF
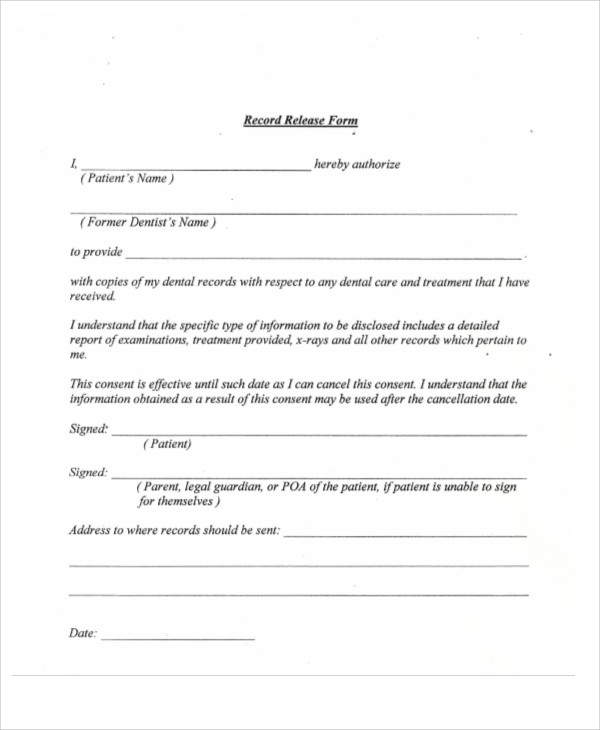
Web the dental records release form is a document that is provided by a dental patient or the parent or guardian of the patient if the patient is a minor, or of proper relations, for the purpose of obtaining dental records from another dentist or dental specialist. Once completed, dental clinics can forward this form to other dentists as proof.
FREE 11+ Sample Dental Release Forms in MS Word PDF
Use the cross or check marks in the top toolbar to select your answers in the list boxes. Web orthodontic records release form patient name first name last name i hereby give my permission to release any/all information pertaining to orthodontic treatment (diagnostic records) and treatment notes for myself/child to the office of dr. To send just this basic information.
FREE 6+ Dental Records Release Forms in PDF MS Word
Invisalign® in honolulu and kailua; Web orthodontic records release form patient name first name last name i hereby give my permission to release any/all information pertaining to orthodontic treatment (diagnostic records) and treatment notes for myself/child to the office of dr. Web 01 to fill out the early removal of braces, you should first consult with your orthodontist or dentist..
This Information Is Necessary For The Dentist To Have The Ability To Review The Previous Records.
Invisalign® in honolulu and kailua; Web the dental records release form is a document that is provided by a dental patient or the parent or guardian of the patient if the patient is a minor, or of proper relations, for the purpose of obtaining dental records from another dentist or dental specialist. Web 01 to fill out the early removal of braces, you should first consult with your orthodontist or dentist. Once completed, dental clinics can forward this form to other dentists as proof of authorization to release their particulars to the clinic.
Web I Understand That This Is A Full Waiver And Release Of Any And All Claims (I) (My Child ___________) Or Anyone Claiming Through Or On Behalf Of (Me) (My Child) May Now Have Or May Acquire In The Future Arising Out Of The Removal Of (My) (My Child’s) Appliances As Aforesaid By Said Doctor, His/Her Agents Or Employees.
Use the cross or check marks in the top toolbar to select your answers in the list boxes. Start completing the fillable fields and carefully type in required information. Web it is necessary that your records be transferred to assure that the receiving orthodontist is knowledgeable of your orthodontic condition(s), orthodontic treatment goals, the current treatment plan, and related financial arrangements. 02 if you are eligible for early removal of braces, your orthodontist or dentist will provide you with the necessary paperwork or forms to fill out.
To Send Just This Basic Information Described Above Please Check Here !
To facilitate the transfer of these records, it is necessary that you complete the following: Web orthodontic records release form patient name first name last name i hereby give my permission to release any/all information pertaining to orthodontic treatment (diagnostic records) and treatment notes for myself/child to the office of dr. They will assess your specific situation and determine if you are a candidate for early removal. Use get form or simply click on the template preview to open it in the editor.