Saxenda Prior Authorization Form
Saxenda Prior Authorization Form - Has the patient completed at least 16 weeks of therapy (saxenda, contrave) or 3 months of therapy at a stable maintenance dose (wegovy)? For saxenda request for chronic weight management in pediatrics, approve. Web • saxenda has not been studied in patients with a history of pancreatitis. Current bmi ≥ 40 kg/m. Saxenda is indicated as an. Web initial authorization • one of the following: Web prior authorization request form for liraglutide 3 mg injection (saxenda) 6. December 09, 2019 urac accredited pharmacy benefit management, expires. Web prior authorization is recommended for prescription benefit coverage of saxenda and wegovy. Web saxenda (liraglutide injection) status:
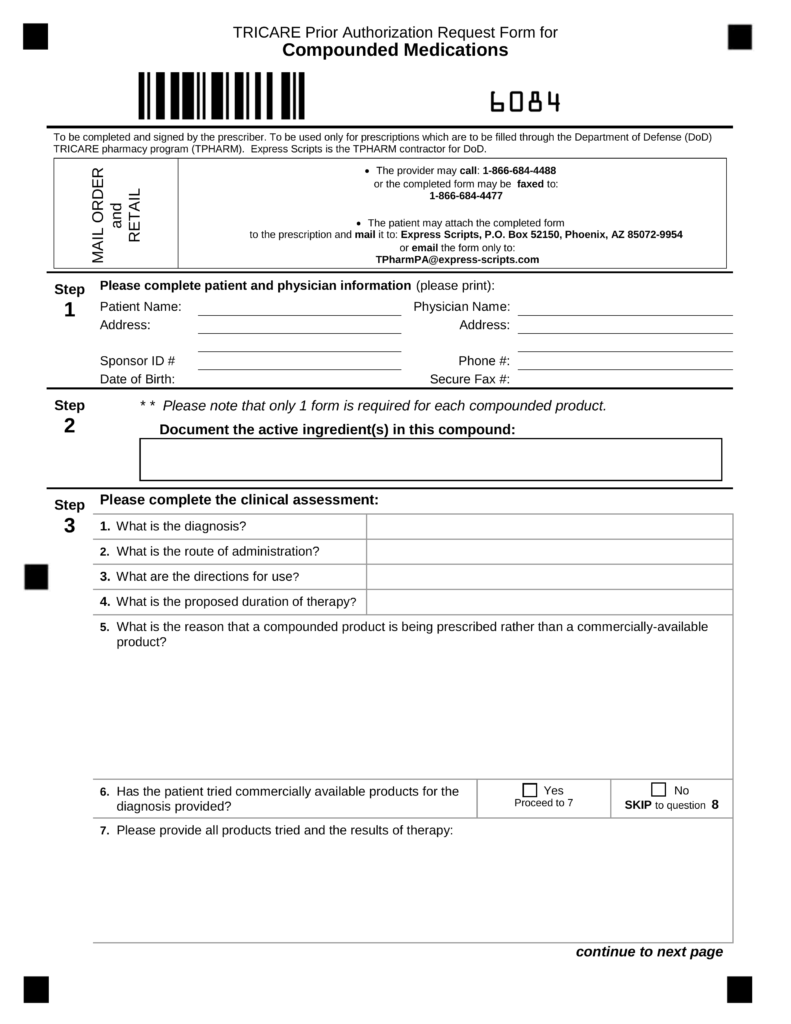
Web saxenda (liraglutide injection) status: Web step please complete patient and physician information (please print): Web coverage request letter coverage request letter are you frustrated because saxenda® (liraglutide) injection 3 mg is not covered by your employer’s prescription benefit plan?. Current bmi ≥ 40 kg/m. Web saxenda (liraglutide injection) status: Prescribers may refer to the forms page of the. Give the form to your provider to complete and send back to express scripts. Sponsor id # phone #: Web prior authorization is recommended for prescription benefit coverage of saxenda and wegovy. Web prior authorization request form for liraglutide 3 mg injection (saxenda) 6.
Novo nordisk collaborates with covermymeds ® for a convenient way to. Saxenda is indicated as an. Of note, this policy targets saxenda and wegovy; For saxenda request for chronic weight management in pediatrics, approve. Initial coverage (*if approved, initial coverage will be for 18 weeks) liraglutide (saxenda) may be eligible for coverage when. Web once you have verified your patient’s benefits, then you can initiate the prior authorization process. Web initial authorization • one of the following: Web how to get medical necessity. Web coverage request letter coverage request letter are you frustrated because saxenda® (liraglutide) injection 3 mg is not covered by your employer’s prescription benefit plan?. Prescribers may refer to the forms page of the.

Prime Therapeutics Prior Authorization Form Pdf amulette
Web once you have verified your patient’s benefits, then you can initiate the prior authorization process. Web prior authorization request form for liraglutide 3 mg injection (saxenda) 6. Web saxenda (liraglutide injection) status: Prescribers may refer to the forms page of the. Web coverage request letter coverage request letter are you frustrated because saxenda® (liraglutide) injection 3 mg is not.

Sun Life Prior Authorization Form Pdf Fill Online, Printable
Web initial authorization • one of the following: Web prior authorization is recommended for prescription benefit coverage of saxenda and wegovy. Web • saxenda has not been studied in patients with a history of pancreatitis. Has the patient completed at least 16 weeks of therapy (saxenda, contrave) or 3 months of therapy at a stable maintenance dose (wegovy)? Sponsor id.
FREE 35+ Sample Authorization Forms in PDF
Download and print the form for your drug. December 09, 2019 urac accredited pharmacy benefit management, expires. Sponsor id # phone #: Novo nordisk collaborates with covermymeds ® for a convenient way to. Current bmi ≥ 40 kg/m.
lyrica free samples
Web prior authorization is recommended for prescription benefit coverage of saxenda and wegovy. Of note, this policy targets saxenda and wegovy; Web step please complete patient and physician information (please print): December 09, 2019 urac accredited pharmacy benefit management, expires. For saxenda request for chronic weight management in pediatrics, approve.

Cvs Caremark Prior Authorization Form For Fill Online, Printable
Web saxenda (liraglutide injection) status: Saxenda is indicated as an. Web coverage request letter coverage request letter are you frustrated because saxenda® (liraglutide) injection 3 mg is not covered by your employer’s prescription benefit plan?. Coverage criteria the requested medication will be covered with prior authorization when the. Web prior authorization is recommended for prescription benefit coverage of saxenda and.

PATIENT HIPAA CONSENT FORM Remedy Weight Loss 20202022 Fill and
Web once you have verified your patient’s benefits, then you can initiate the prior authorization process. Download and print the form for your drug. Web step please complete patient and physician information (please print): Initial coverage (*if approved, initial coverage will be for 18 weeks) liraglutide (saxenda) may be eligible for coverage when. Coverage criteria the requested medication will be.
Colorful Strings Isolated On White Background Stock Image Image of
Novo nordisk collaborates with covermymeds ® for a convenient way to. Coverage criteria the requested medication will be covered with prior authorization when the. Web tricare prior authorization request form for liraglutide 3 mg injection (saxenda), semaglutide 2.4mg injection (wegovy) to be completed and signed by the prescriber. Of note, this policy targets saxenda and wegovy; For saxenda request for.

Bcbs Prior Authorization Form Tennessee Form Resume Examples
Give the form to your provider to complete and send back to express scripts. Saxenda is indicated as an. Of note, this policy targets saxenda and wegovy; Web tricare prior authorization request form for liraglutide 3 mg injection (saxenda), semaglutide 2.4mg injection (wegovy) to be completed and signed by the prescriber. Web • saxenda has not been studied in patients.
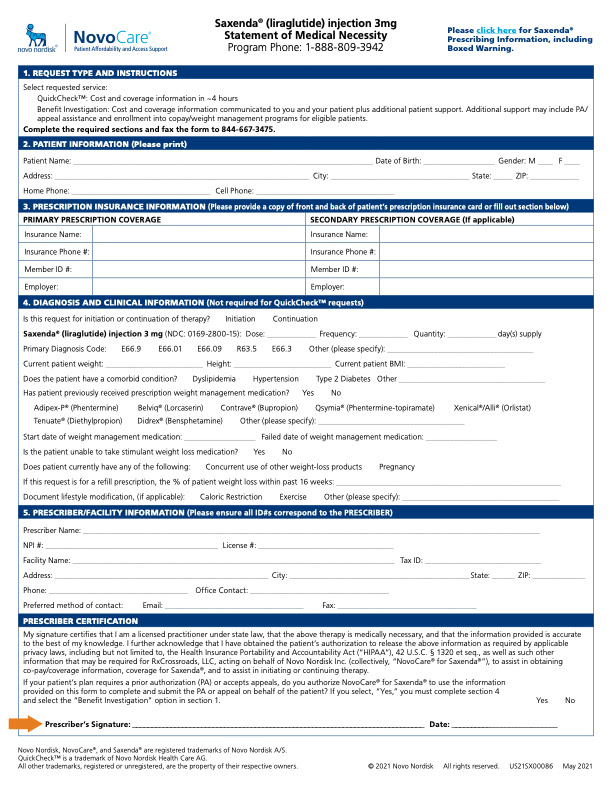
Saxenda® (liraglutide) Injection 3 mg Coverage
Prescribers may refer to the forms page of the. Web how to get medical necessity. Web saxenda (liraglutide injection) status: Web once you have verified your patient’s benefits, then you can initiate the prior authorization process. Web initial authorization • one of the following:

Medicare Generation Rx Prior Authorization Form Form Resume
Saxenda is indicated as an. Web coverage request letter coverage request letter are you frustrated because saxenda® (liraglutide) injection 3 mg is not covered by your employer’s prescription benefit plan?. Initial coverage (*if approved, initial coverage will be for 18 weeks) liraglutide (saxenda) may be eligible for coverage when. Web tricare prior authorization request form for liraglutide 3 mg injection.
Download And Print The Form For Your Drug.
Web saxenda (liraglutide injection) status: Web step please complete patient and physician information (please print): Novo nordisk collaborates with covermymeds ® for a convenient way to. Web tricare prior authorization request form for liraglutide 3 mg injection (saxenda), semaglutide 2.4mg injection (wegovy) to be completed and signed by the prescriber.
Yes Or No If Yes To Question 1 And.
Initial coverage (*if approved, initial coverage will be for 18 weeks) liraglutide (saxenda) may be eligible for coverage when. Web initial authorization • one of the following: Prescribers may refer to the forms page of the. Web prior authorization request form for liraglutide 3 mg injection (saxenda) 6.
Coverage Criteria The Requested Medication Will Be Covered With Prior Authorization When The.
Current bmi ≥ 40 kg/m. Web prior authorization is recommended for prescription benefit coverage of saxenda and wegovy. Give the form to your provider to complete and send back to express scripts. Web once you have verified your patient’s benefits, then you can initiate the prior authorization process.
For Saxenda Request For Chronic Weight Management In Pediatrics, Approve.
Sponsor id # phone #: Saxenda is indicated as an. Of note, this policy targets saxenda and wegovy; Web • saxenda has not been studied in patients with a history of pancreatitis.