Vsp Claim Form Pdf
Vsp Claim Form Pdf - Patient information (required) other accident. Web how do i submit a claim? Box 495918 cincinnati, oh 45249. Contact member services at 800.877.7195 for help submitting a claim online or by mail. Fill out your personal information including name, address, and date of birth. Online by mail it’s the way to. Benefits in the navigation or. The easiest way to modify vsp claim form printable in pdf. Web video instructions and help with filling out and completing vsp member reimbursement form pdf. Web there are no claim forms to fill out when you see a vsp network doctor.
Web there are no claim forms to fill out when you see a vsp network doctor. Box 495918 cincinnati, oh 45249. You can also download it, export it or print it out. Web video instructions and help with filling out and completing vsp member reimbursement form pdf. Read all the field labels carefully. Fill out your personal information including name, address, and date of birth. Web mail the completed claim form to: Web up to $40 cash back 1. Patient information (required) other accident. Web send vsp member reimbursement form via email, link, or fax.
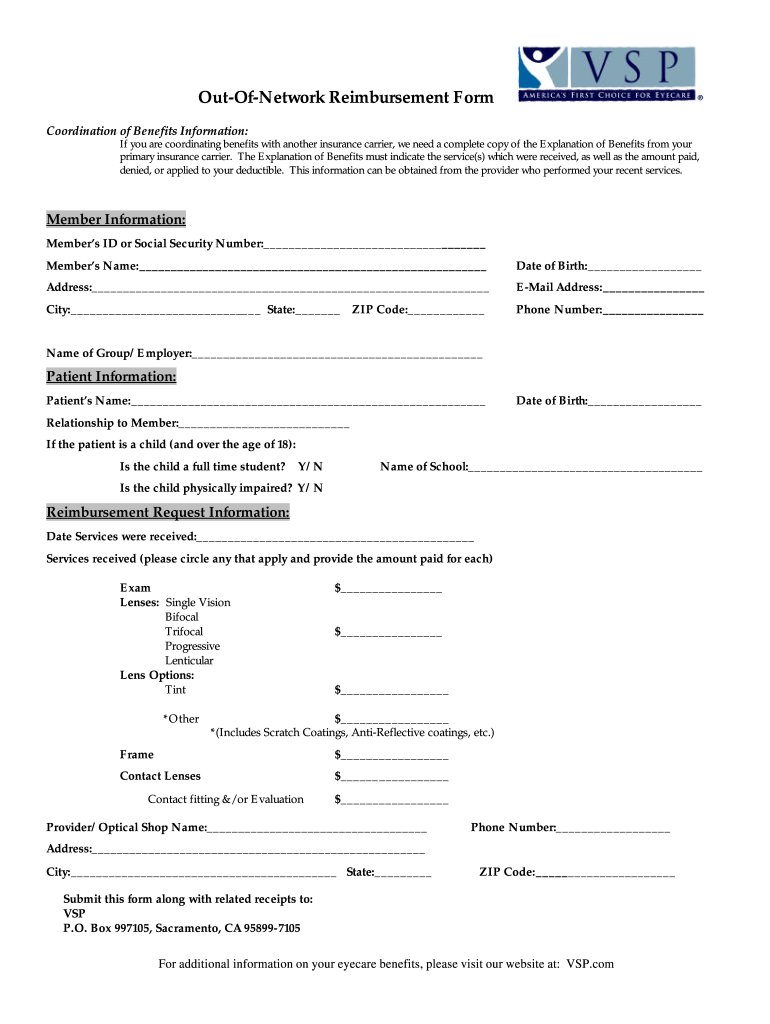
Web vsp member reimbursement form to request reimbursement, complete this form (in blue or black ink), enclose a legible copy of your itemized receipt(s) and send them to the. Web mail the completed claim form to: Web vsp member reimbursement form to request reimbursement, complete this form (in blue or black ink), enclose a legible copy of your itemized receipt(s), and send them to. Web complete vsp reimbursement form online with us legal forms. Before your next visit, find a vsp network doctor near you to help keep your eyes healthy and your wallet. Web vsp vision care | vision insurance. Be sure to keep a. Benefits in the navigation or. Contact member services at 800.877.7195 for help submitting a claim online or by mail. Web send vsp member reimbursement form via email, link, or fax.

Vsp Claim Form Printable Printable Word Searches
The easiest way to modify vsp claim form printable in pdf. Web mail the completed claim form to: Web vsp member reimbursement form to request reimbursement, complete this form (in blue or black ink), enclose a legible copy of your itemized receipt(s), and send them to. Read all the field labels carefully. We are here to help.

Fill Free fillable VSP Member Reimbursement Form
Web vsp vision care | vision insurance. This site uses cookies and related technologies to operate our site, help keep you safe, improve your experience, perform. Go digital and save time with signnow, the best. Web to request reimbursement, complete this form (in blue or black ink), enclose a legible copy of your itemized receipt(s), and send them to the.
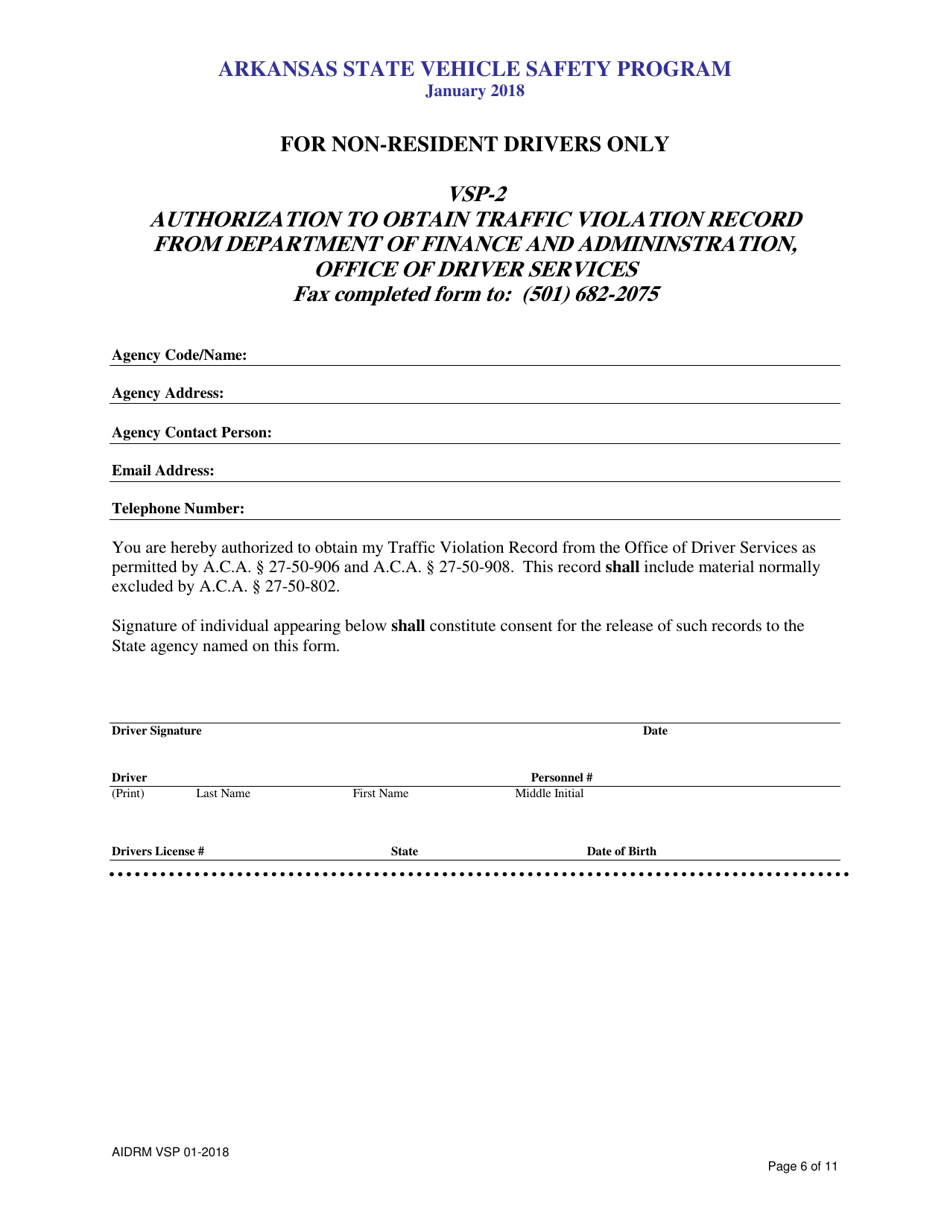
Form VSP2 Download Printable PDF or Fill Online Authorization to
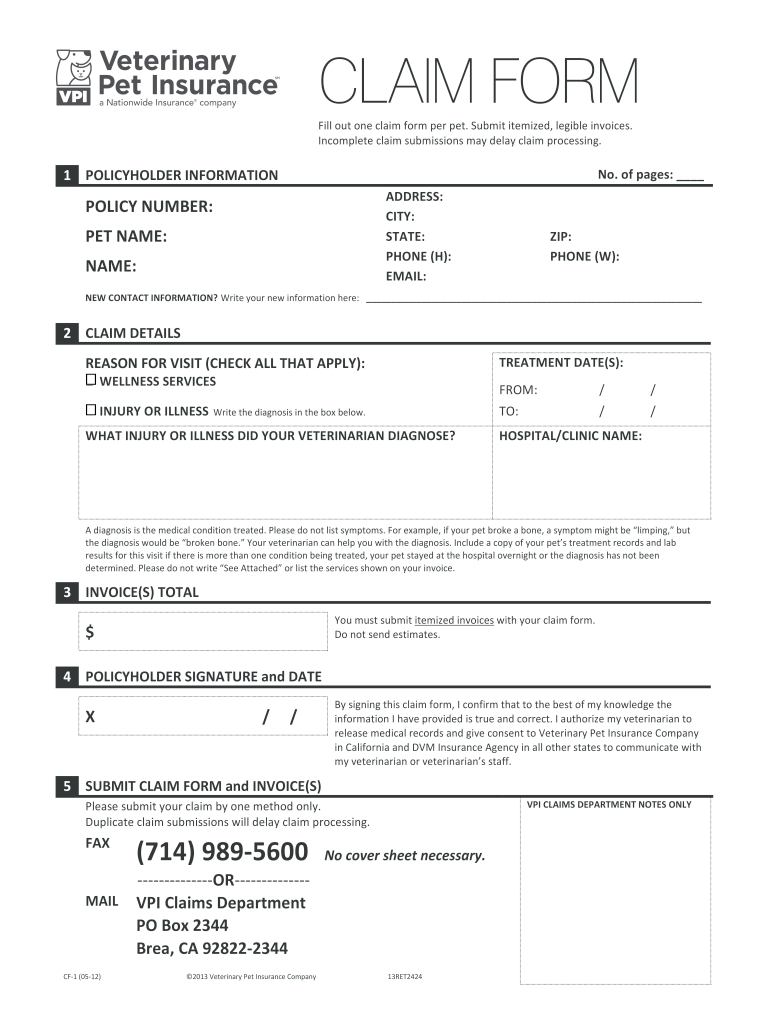
Web vsp vision care | vision insurance. Find a suitable template on the internet. Your doctor will take care of the claims process for you. Web there are no claim forms to fill out when you see a vsp network doctor. Web when you see a vsp network doctor or provider, there are no claim forms to complete.
Vsp Claim Form Fill Out and Sign Printable PDF Template signNow
Web when you see a vsp network doctor or provider, there are no claim forms to complete. Easily fill out pdf blank, edit, and sign them. Web there are no claim forms to fill out when you see a vsp network doctor. Web claims and reimbursement submit a claim how do i submit a claim? Web up to $40 cash.
Vsp Claim Forms Fill Out and Sign Printable PDF Template signNow
Patient information (required) other accident. Web vsp vision care | vision insurance. Web send vsp member reimbursement form via email, link, or fax. Save or instantly send your ready documents. Web there are no claim forms to fill out when you see a vsp network doctor.
Use Vision Insurance & FSAs/HSAs for Eyewear
Find a suitable template on the internet. Web claims and reimbursement submit a claim how do i submit a claim? Web vsp member reimbursement form to request reimbursement, complete this form (in blue or black ink), enclose a legible copy of your itemized receipt(s), and send them to. Easily fill out pdf blank, edit, and sign them. The easiest way.

Form DEP6064 Download Printable PDF or Fill Online Claim Request Form
Web vsp vision care | vision insurance. Find a suitable template on the internet. Go digital and save time with signnow, the best. Box 495918 cincinnati, oh 45249. Read all the field labels carefully.
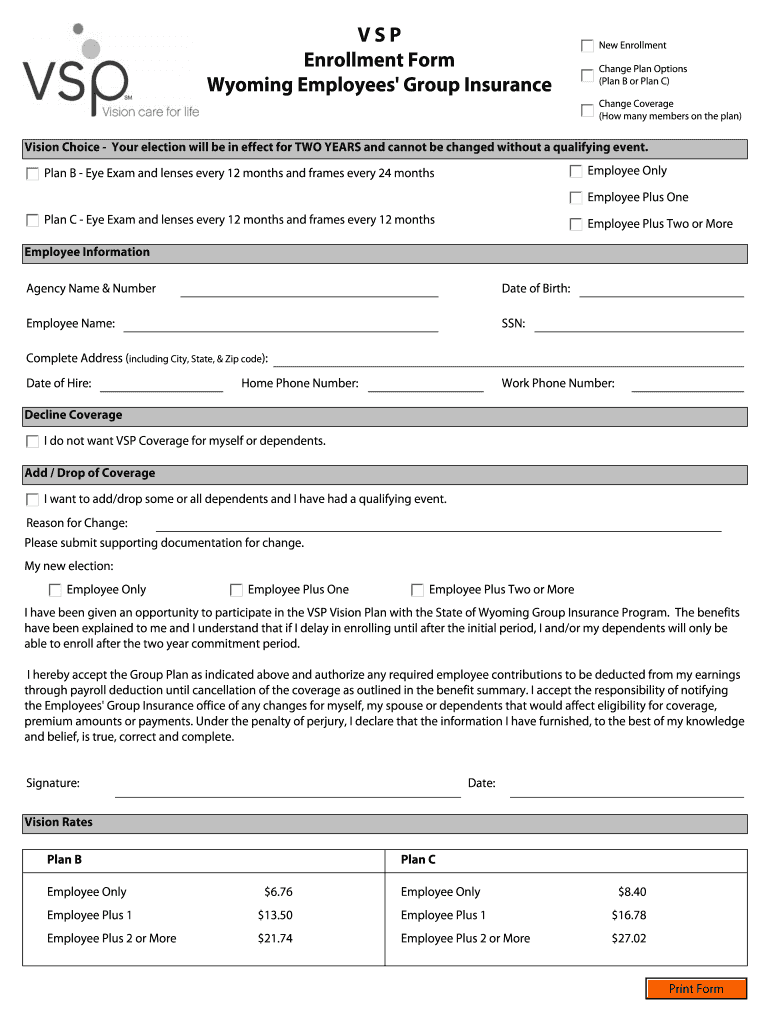
Vsp Enrollment Form Pdf Fill Online, Printable, Fillable, Blank
Download the vsp reimbursement form from the vsp website. Your doctor will take care of the claims process for you. Web there are no claim forms to fill out when you see a vsp network doctor. Web video instructions and help with filling out and completing vsp member reimbursement form pdf. Web vsp member reimbursement form to request reimbursement, complete.
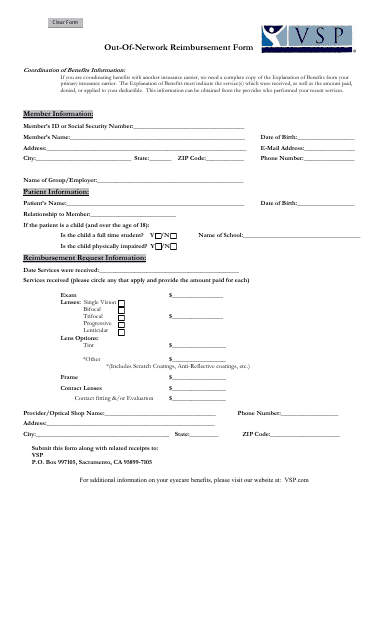
California Out of Network Reimbursement Form Vsp Download Fillable
Contact member services at 800.877.7195 for help submitting a claim online or by mail. Web claims and reimbursement submit a claim how do i submit a claim? Web complete vsp reimbursement form online with us legal forms. Easily fill out pdf blank, edit, and sign them. Web when you see a vsp network doctor or provider, there are no claim.
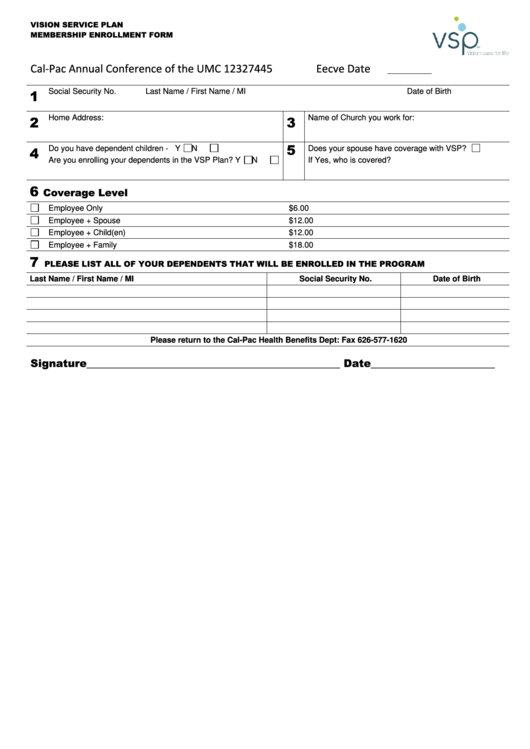
Vsp Client Enrollment Form printable pdf download
Web complete vsp reimbursement form online with us legal forms. Be sure to keep a. Web mail the completed claim form to: Go digital and save time with signnow, the best. Save or instantly send your ready documents.
Contact Member Services At 800.877.7195 For Help Submitting A Claim Online Or By Mail.
Patient information (required) other accident. The easiest way to modify vsp claim form printable in pdf. Before your next visit, find a vsp network doctor near you to help keep your eyes healthy and your wallet. Your doctor will take care of the claims process for you.
Web Vsp Vision Care | Vision Insurance.
Web video instructions and help with filling out and completing vsp member reimbursement form pdf. Web send vsp member reimbursement form via email, link, or fax. Save or instantly send your ready documents. Benefits in the navigation or.
Go Digital And Save Time With Signnow, The Best.
We are here to help. Web how do i submit a claim? Be sure to keep a. Box 495918 cincinnati, oh 45249.
Web To Request Reimbursement, Complete This Form (In Blue Or Black Ink), Enclose A Legible Copy Of Your Itemized Receipt(S), And Send Them To The Following Address.
Web when you see a vsp network doctor or provider, there are no claim forms to complete. Read all the field labels carefully. Web vsp vision care | vision insurance. This site uses cookies and related technologies to operate our site, help keep you safe, improve your experience, perform.