Arcalyst Enrollment Form
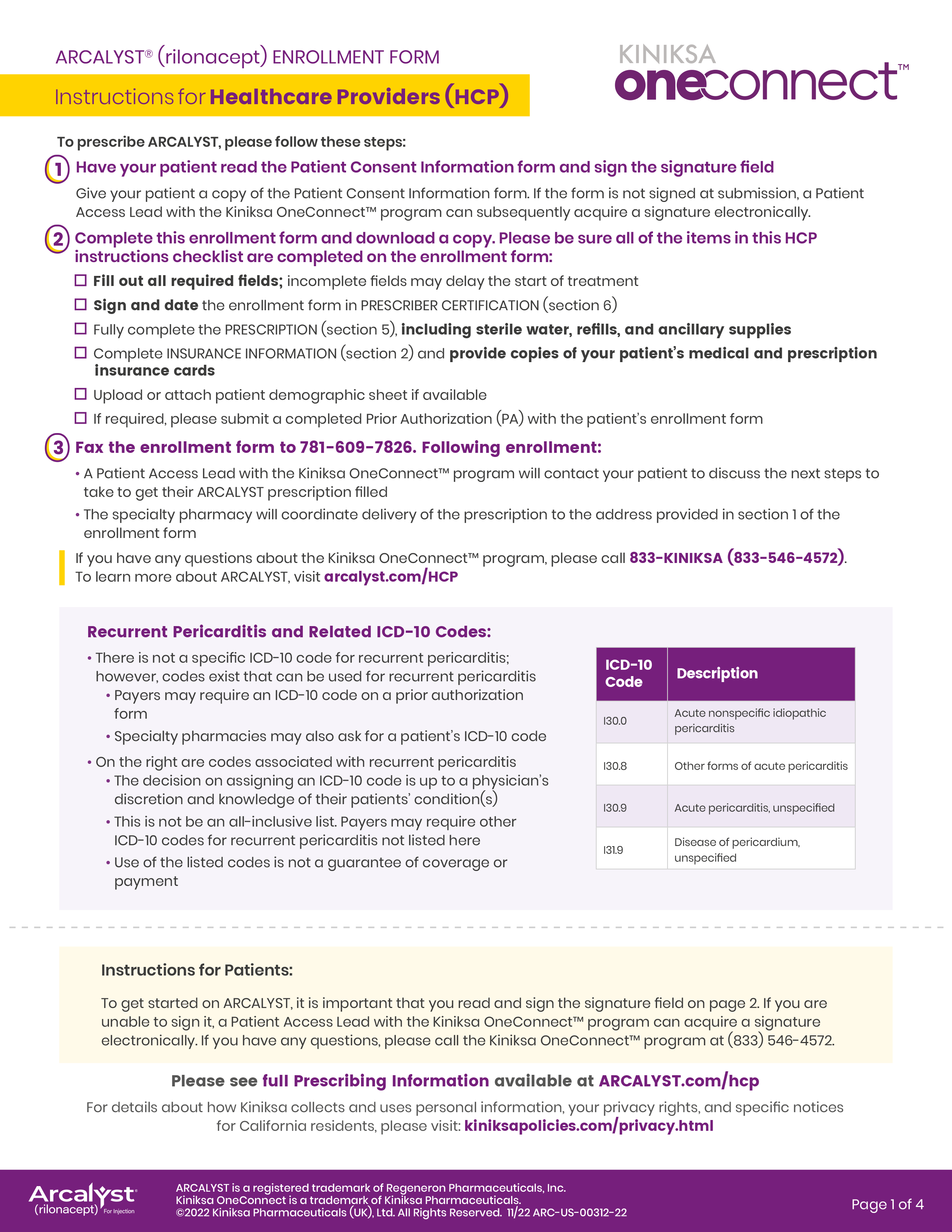
Arcalyst Enrollment Form - Recurrent pericarditis (english) recurrent pericarditis (spanish) caps/dira; Web if required, please submit a completed prior authorization (pa) with the patient’s enrollment form. Web please print and complete the forms below. Web the enrollment form will be provided by your kiniksa sales specialist or is available for download below. Fax the enrollment form to. Web instructions for patients to get started on arcalyst, please follow these steps: Once completed, fax to the number indicated on the form. Referral forms for arcalyst® (rilonacept): Web arcalyst® (rilonacept) enrollment form instructions for healthcare providers (hcp) to prescribe arcalyst, please follow these steps: Web enrollment form completion enrollment form will be provided by your kiniksa clinical sales specialist or available for download below.
Web if required, please submit a completed prior authorization (pa) with the patient’s enrollment form. Fax the enrollment form to. Once completed, fax to the number indicated on the form. We will help make the start of your treatment a seamless experience. Web the enrollment form will be provided by your kiniksa sales specialist or is available for download below. Recurrent pericarditis (rp) or other indication enrollment form. Web most recent arcalyst prior authorization forms. Referral forms for arcalyst® (rilonacept): Web instructions for patients to get started on arcalyst, please follow these steps: Read the patient consent information and sign the 3 signature fields your healthcare provider will fill out the enrollment form following enrollment:
Recurrent pericarditis (english) recurrent pericarditis (spanish) caps/dira; Once completed, fax to the number indicated on the form. Web arcalyst® (rilonacept) enrollment form instructions for healthcare providers (hcp) to prescribe arcalyst, please follow these steps: Web if required, please submit a completed prior authorization (pa) with the patient’s enrollment form. Web please print and complete the forms below. Referral forms for arcalyst® (rilonacept): Read the patient consent information and sign the 3 signature fields your healthcare provider will fill out the enrollment form following enrollment: We will help make the start of your treatment a seamless experience. Web enrollment form completion enrollment form will be provided by your kiniksa clinical sales specialist or available for download below. Web instructions for patients to get started on arcalyst, please follow these steps:

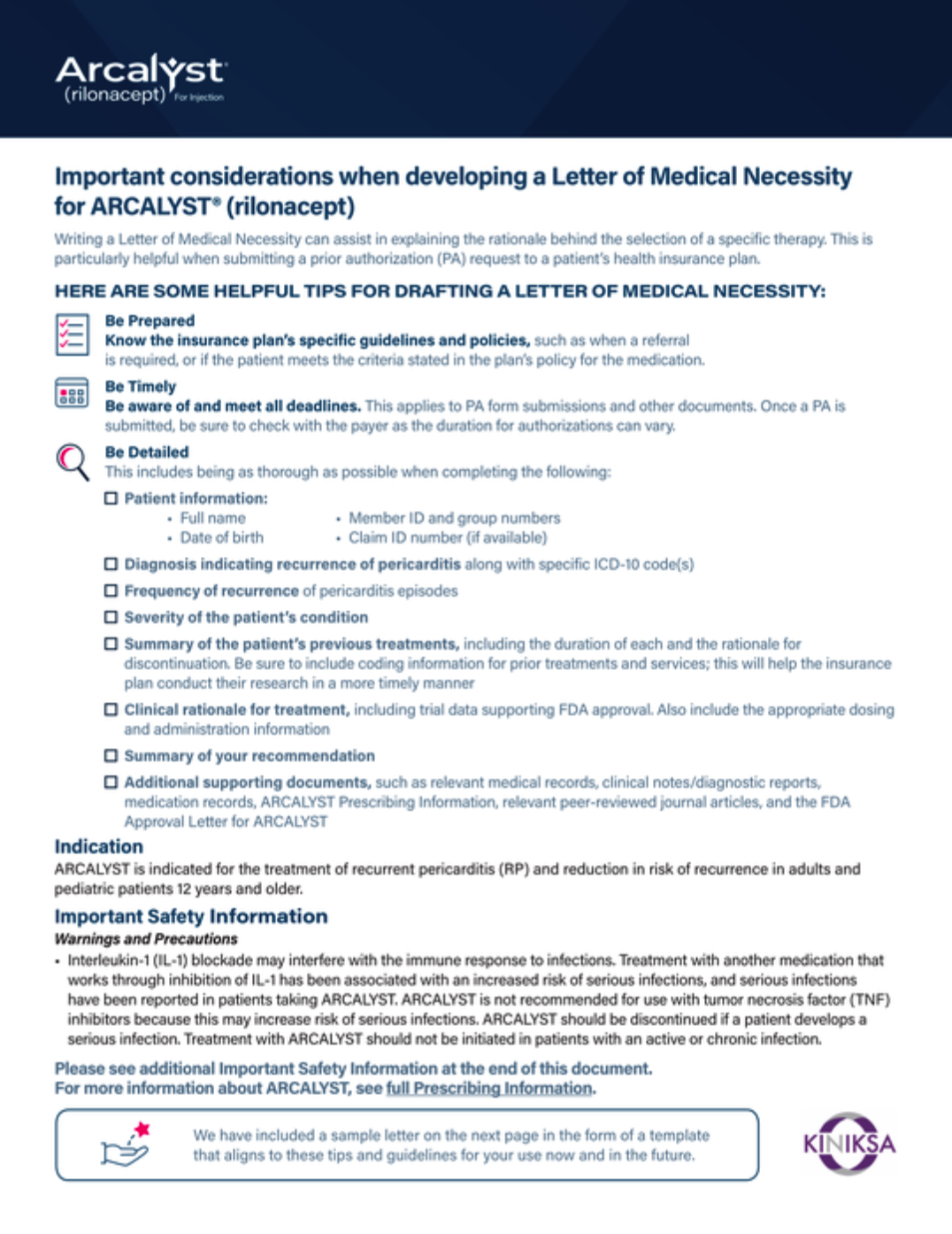
Arcalyst FDA prescribing information, side effects and uses
Fax the enrollment form to. 1 your patient read the patient consent information form and sign the signature field give your patient a copy of the patient consent information form. Once completed, fax to the number indicated on the form. Web most recent arcalyst prior authorization forms. Web enrollment form completion enrollment form will be provided by your kiniksa clinical.
Access Information ARCALYST (rilonacept)
Fax the enrollment form to. Web the enrollment form will be provided by your kiniksa sales specialist or is available for download below. Web enrollment form completion enrollment form will be provided by your kiniksa clinical sales specialist or available for download below. Web most recent arcalyst prior authorization forms. Web instructions for patients to get started on arcalyst, please.
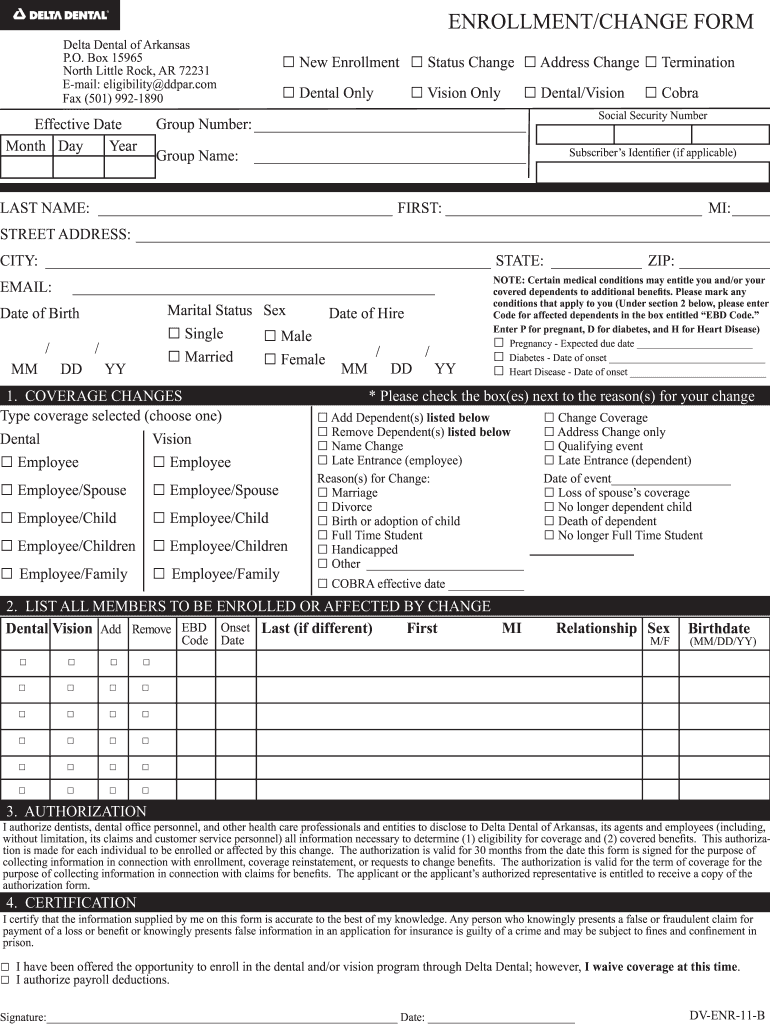
Delta Dental Enrollment Form Fill Out and Sign Printable PDF Template
Recurrent pericarditis (rp) or other indication enrollment form. We will help make the start of your treatment a seamless experience. Web please print and complete the forms below. Web after your healthcare provider submits a kiniksa oneconnect ™ enrollment form with your signature and consent, our work begins. Fax the enrollment form to.
Access and Support ARCALYST (rilonacept)
Read the patient consent information and sign the 3 signature fields your healthcare provider will fill out the enrollment form following enrollment: Web after your healthcare provider submits a kiniksa oneconnect ™ enrollment form with your signature and consent, our work begins. Web the enrollment form will be provided by your kiniksa sales specialist or is available for download below..
Access and Support ARCALYST (rilonacept)
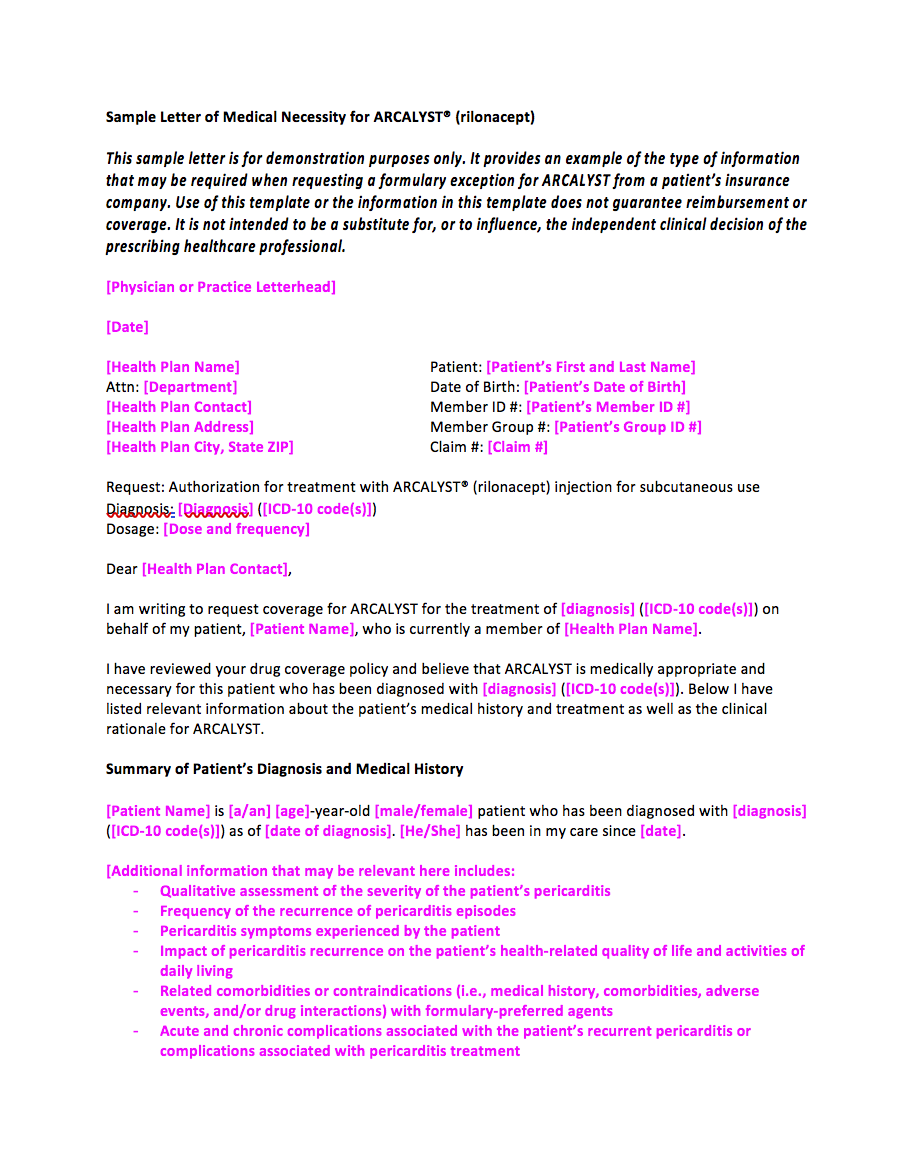
Web arcalyst® (rilonacept) enrollment form instructions for healthcare providers (hcp) to prescribe arcalyst, please follow these steps: Recurrent pericarditis (rp) or other indication enrollment form. Web the enrollment form will be provided by your kiniksa sales specialist or is available for download below. Web if required, please submit a completed prior authorization (pa) with the patient’s enrollment form. We will.
Enrollment Forms MUST be Returned by June 15 Announce University of
Web instructions for patients to get started on arcalyst, please follow these steps: Web enrollment form completion enrollment form will be provided by your kiniksa clinical sales specialist or available for download below. We will help make the start of your treatment a seamless experience. Recurrent pericarditis (english) recurrent pericarditis (spanish) caps/dira; Fax the enrollment form to.
Access and Support ARCALYST (rilonacept)
Web most recent arcalyst prior authorization forms. Web if required, please submit a completed prior authorization (pa) with the patient’s enrollment form. Recurrent pericarditis (english) recurrent pericarditis (spanish) caps/dira; Read the patient consent information and sign the 3 signature fields your healthcare provider will fill out the enrollment form following enrollment: Web after your healthcare provider submits a kiniksa oneconnect.

Kiniksa Wins FDA Nod For ARCALYST Injection therapy; Shares Pop After
1 your patient read the patient consent information form and sign the signature field give your patient a copy of the patient consent information form. We will help make the start of your treatment a seamless experience. Recurrent pericarditis (english) recurrent pericarditis (spanish) caps/dira; Web please print and complete the forms below. Web instructions for patients to get started on.

Safety and Administration ARCALYST (rilonacept)
Recurrent pericarditis (english) recurrent pericarditis (spanish) caps/dira; Read the patient consent information and sign the 3 signature fields your healthcare provider will fill out the enrollment form following enrollment: Once completed, fax to the number indicated on the form. We will help make the start of your treatment a seamless experience. Recurrent pericarditis (rp) or other indication enrollment form.

FREE 8+ Sample Enrollment Forms in PDF MS Word
Read the patient consent information and sign the 3 signature fields your healthcare provider will fill out the enrollment form following enrollment: Referral forms for arcalyst® (rilonacept): Once completed, fax to the number indicated on the form. Fax the enrollment form to. Web please print and complete the forms below.
Web Instructions For Patients To Get Started On Arcalyst, Please Follow These Steps:
Fax the enrollment form to. Web enrollment form completion enrollment form will be provided by your kiniksa clinical sales specialist or available for download below. Referral forms for arcalyst® (rilonacept): Once completed, fax to the number indicated on the form.
Web Most Recent Arcalyst Prior Authorization Forms.
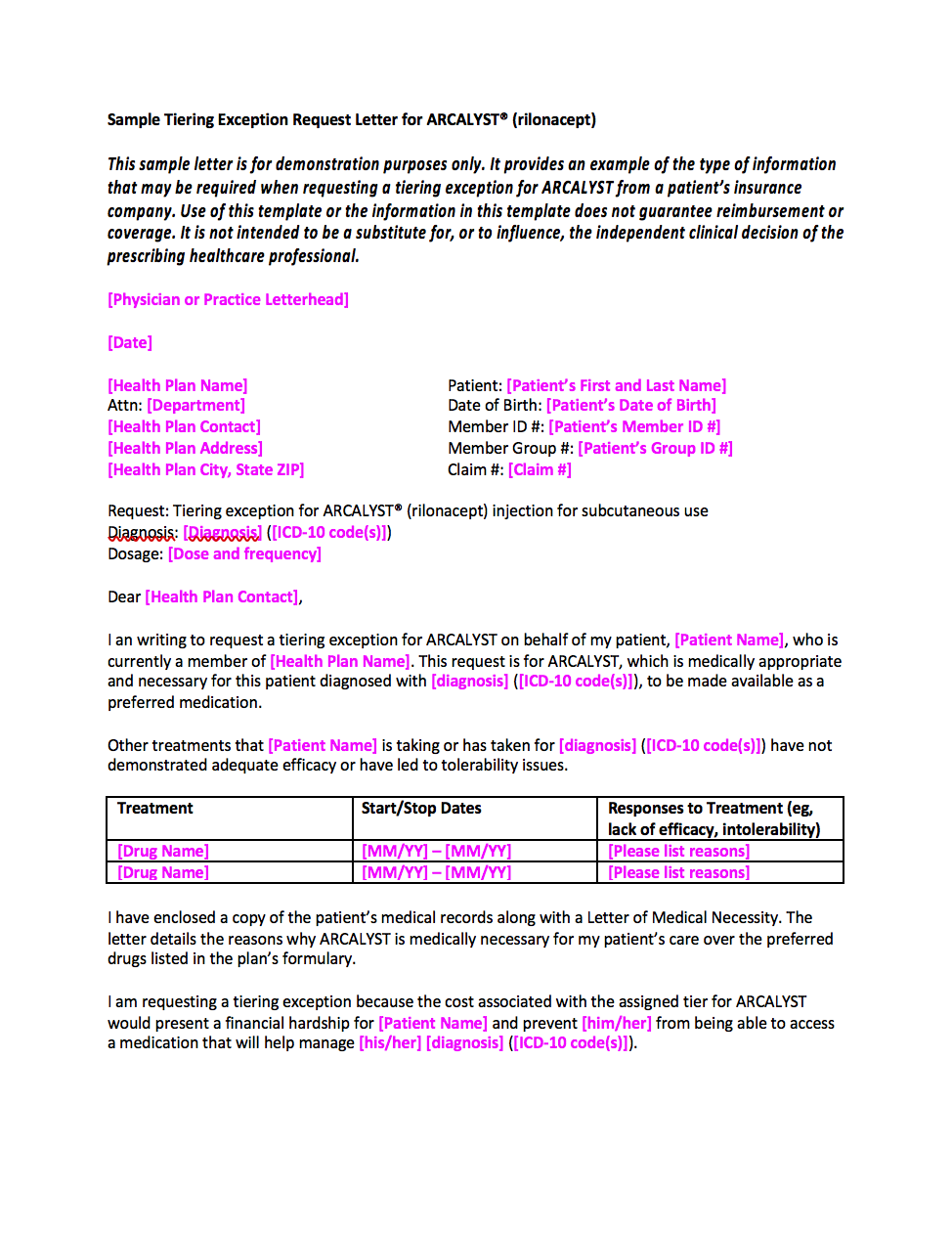
Web arcalyst® (rilonacept) enrollment form instructions for healthcare providers (hcp) to prescribe arcalyst, please follow these steps: Web the enrollment form will be provided by your kiniksa sales specialist or is available for download below. Web please print and complete the forms below. Web if required, please submit a completed prior authorization (pa) with the patient’s enrollment form.
1 Your Patient Read The Patient Consent Information Form And Sign The Signature Field Give Your Patient A Copy Of The Patient Consent Information Form.
Web after your healthcare provider submits a kiniksa oneconnect ™ enrollment form with your signature and consent, our work begins. Read the patient consent information and sign the 3 signature fields your healthcare provider will fill out the enrollment form following enrollment: Recurrent pericarditis (rp) or other indication enrollment form. We will help make the start of your treatment a seamless experience.