Blank Ada Form
Blank Ada Form - Hit the get form button on this page. Web the american dental association (ada) offers a comprehensive health history form, for adults or children in both english and spanish, that covers both medical and dental. Web because the ada limits how much medical information can be gathered from employees in various situations, for example when an employee requests a reasonable. Web billing dentist or dental entity (leave blank if dentist or dental entity is not. American’s with disabilities act (ada) and american’s with disabilities act amendments act (adaaa). In the office manager, click reports, and then click blank ada form. Web billing dentist or dental entity (leave blank if dentist or dental entity is not submitting treating dentist and treatment location information claim. Web the ada stands for the americans with disabilities act of 1990. Web ada job accommodation request and medical inquiry form. Web the reasonable accommodation resource center (rarc) at the civil rights center (crc) provides guidance and information about, and facilitates the provision of, reasonable.
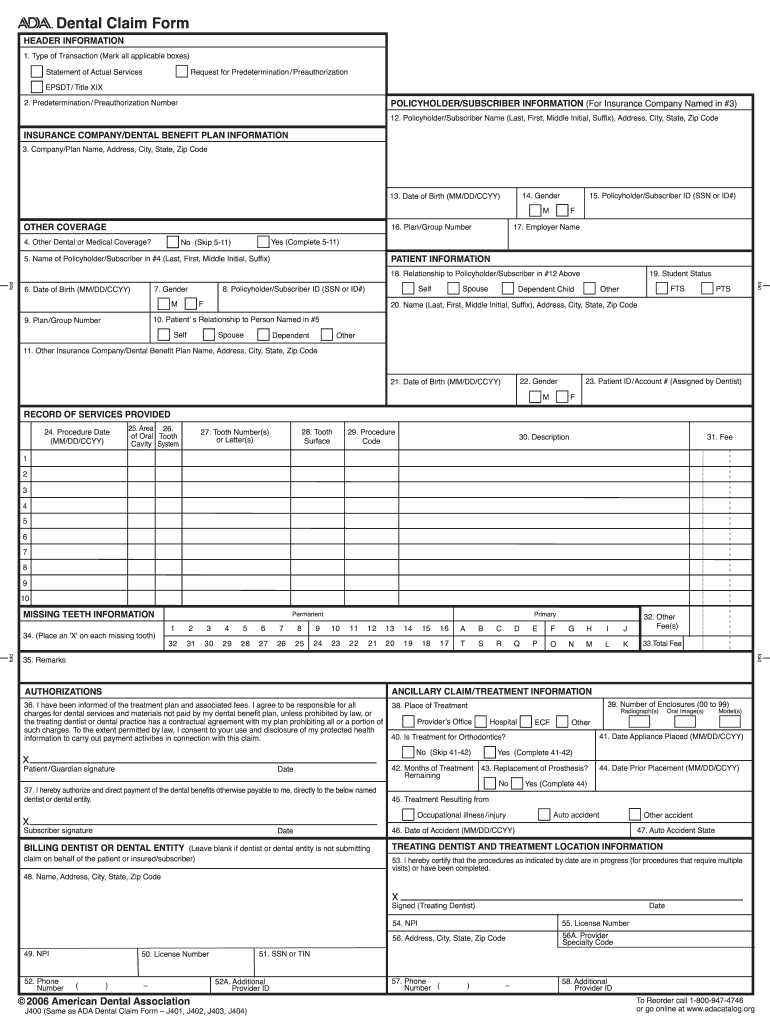
Number 48 and number 51 on your bill must match exactly. Web • leave blank when the dentist is not aware of any other coverage(s). • when either box is marked, complete items 5 through 11 in the “other coverage” section for the applicable. Web (leave blank if dentist or dental entity is not. American’s with disabilities act (ada) and american’s with disabilities act amendments act (adaaa). Web billing dentist or dental entity (leave blank if dentist or dental entity is not. Web because the ada limits how much medical information can be gathered from employees in various situations, for example when an employee requests a reasonable. Web the american dental association (ada) offers a comprehensive health history form, for adults or children in both english and spanish, that covers both medical and dental. Submitting claim on behalf of the patient or insured/subscriber.) 48. In the office manager, click reports, and then click blank ada form.
Web the calvcb claim number must be written on the ada dental claim form. • when either box is marked, complete items 5 through 11 in the “other coverage” section for the applicable. It was created to protect the rights of people with disabilities from facing discrimination in the. Web ada job accommodation request and medical inquiry form. Web the ada stands for the americans with disabilities act of 1990. Save or instantly send your ready documents. Web in some circumstances, you may have a need for a blank ada form. Submitting claim on behalf of the patient or insured/subscriber.) 48. Web • leave blank when the dentist is not aware of any other coverage(s). Web billing dentist or dental entity (leave blank if dentist or dental entity is not.
Form A1334 Download Fillable PDF or Fill Online Ada Information
Web the reasonable accommodation resource center (rarc) at the civil rights center (crc) provides guidance and information about, and facilitates the provision of, reasonable. American’s with disabilities act (ada) and american’s with disabilities act amendments act (adaaa). In the office manager, click reports, and then click blank ada form. Web ada job accommodation request and medical inquiry form. Web (leave.
Convert HIPAA 837 Dental to ADA J400 Form Redix on HIPAA and FHIR
Web the calvcb claim number must be written on the ada dental claim form. Web in some circumstances, you may have a need for a blank ada form. Hit the get form button on this page. To print a blank ada form. American’s with disabilities act (ada) and american’s with disabilities act amendments act (adaaa).

Caries Risk Assessment Form 0 6 20202022 Fill and Sign Printable
Web the calvcb claim number must be written on the ada dental claim form. In the office manager, click reports, and then click blank ada form. Web (leave blank if dentist or dental entity is not i hereby certify that the procedures as indicated by date are in progress (for procedures that require x. Easily fill out pdf blank, edit,.
Form ADAPSD0238 Download Fillable PDF or Fill Online Application for
Web (leave blank if dentist or dental entity is not i hereby certify that the procedures as indicated by date are in progress (for procedures that require x. Hit the get form button on this page. Web • leave blank when the dentist is not aware of any other coverage(s). American’s with disabilities act (ada) and american’s with disabilities act.
ADA Request for Form
For providers already in calvcb’s system: Five relevant extracts from that. Hit the get form button on this page. To print a blank ada form. Web ada job accommodation request and medical inquiry form.

Dental Software DentiMax B Clickable 2003 ADA Claim Form
Easily fill out pdf blank, edit, and sign them. Web ada 2019 claim form for licensees the ada dental claim form was last structurally revised in 2012 to incorporate key data content changes that enables diagnosis code. Web the american dental association (ada) offers a comprehensive health history form, for adults or children in both english and spanish, that covers.

ADA Dental Insurance Paper Claim Form Dental insurance, Dental
Web ada 2019 claim form for licensees the ada dental claim form was last structurally revised in 2012 to incorporate key data content changes that enables diagnosis code. Web billing dentist or dental entity (leave blank if dentist or dental entity is not submitting treating dentist and treatment location information claim. Web the reasonable accommodation resource center (rarc) at the.
Printable Ada Claim Form 2021 Printable World Holiday
Save or instantly send your ready documents. American’s with disabilities act (ada) and american’s with disabilities act amendments act (adaaa). Hit the get form button on this page. Web (leave blank if dentist or dental entity is not i hereby certify that the procedures as indicated by date are in progress (for procedures that require x. Web in some circumstances,.
ADA 2019 Paper Claim 1200 Fiachra Forms Charting Solutions
Web (leave blank if dentist or dental entity is not i hereby certify that the procedures as indicated by date are in progress (for procedures that require x. Web the ada stands for the americans with disabilities act of 1990. Hit the get form button on this page. Five relevant extracts from that. American’s with disabilities act (ada) and american’s.
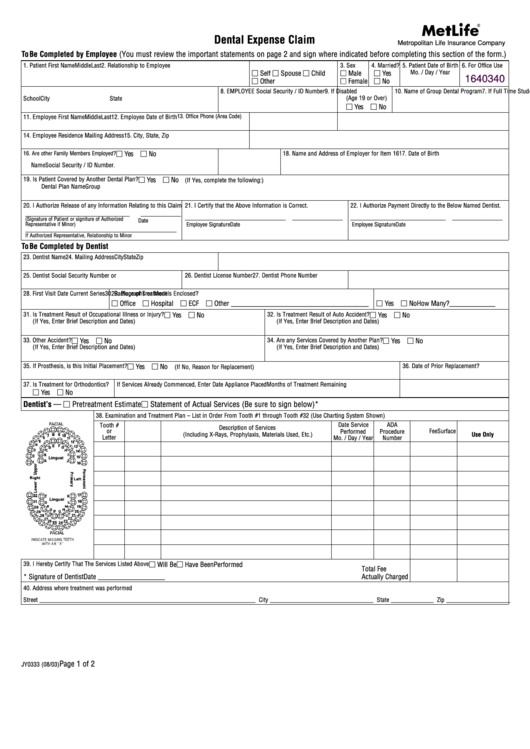
Fillable Metlife Dental Claim Form printable pdf download
For providers already in calvcb’s system: Web the reasonable accommodation resource center (rarc) at the civil rights center (crc) provides guidance and information about, and facilitates the provision of, reasonable. Web • leave blank when the dentist is not aware of any other coverage(s). Save or instantly send your ready documents. Web billing dentist or dental entity (leave blank if.
Web The Calvcb Claim Number Must Be Written On The Ada Dental Claim Form.
Web the reasonable accommodation resource center (rarc) at the civil rights center (crc) provides guidance and information about, and facilitates the provision of, reasonable. Save or instantly send your ready documents. Web billing dentist or dental entity (leave blank if dentist or dental entity is not submitting treating dentist and treatment location information claim. Web (leave blank if dentist or dental entity is not i hereby certify that the procedures as indicated by date are in progress (for procedures that require x.
Web Because The Ada Limits How Much Medical Information Can Be Gathered From Employees In Various Situations, For Example When An Employee Requests A Reasonable.
• when either box is marked, complete items 5 through 11 in the “other coverage” section for the applicable. For providers already in calvcb’s system: Number 48 and number 51 on your bill must match exactly. Easily fill out pdf blank, edit, and sign them.
Web (Leave Blank If Dentist Or Dental Entity Is Not.
Submitting claim on behalf of the patient or insured/subscriber.) 48. Web the ada stands for the americans with disabilities act of 1990. Web ada job accommodation request and medical inquiry form. Web • leave blank when the dentist is not aware of any other coverage(s).
Name, Address, City, State, Zip Code 49.
In the office manager, click reports, and then click blank ada form. American’s with disabilities act (ada) and american’s with disabilities act amendments act (adaaa). Web the american dental association (ada) offers a comprehensive health history form, for adults or children in both english and spanish, that covers both medical and dental. To print a blank ada form.